Over time my experiences have been shifting from young children in schools to elderly in hospice care. It remains as true as it ever was that I am very much learning how to listen, what to say and why. A conversation happened recently though that I thought I would write out in the hopes that it may nurture creative solutions with others.
I was visiting a woman whose diagnosis I do not know (it doesn’t really matter). When I arrived, she was asleep and since she is very hard of hearing, I anticipated that she would rest soundly. Instead of trying to talk with her, I sat down to write her a note. This was the first time she was wearing her hearing aids when I came by and maybe because of that or maybe it was just coincidence, but she woke up.
Her facial expression was confused and worried. She said, ‘I don’t have any money.” Before I could respond, she said more in a rush — much of it a jumble of sounds rather than distinct words. In the mix, I understood, “so sad,” and “but my leg is tangled.”
This is what I said in response:
My goal is to say my name every time because it is not relevant whether or not it is remembered.
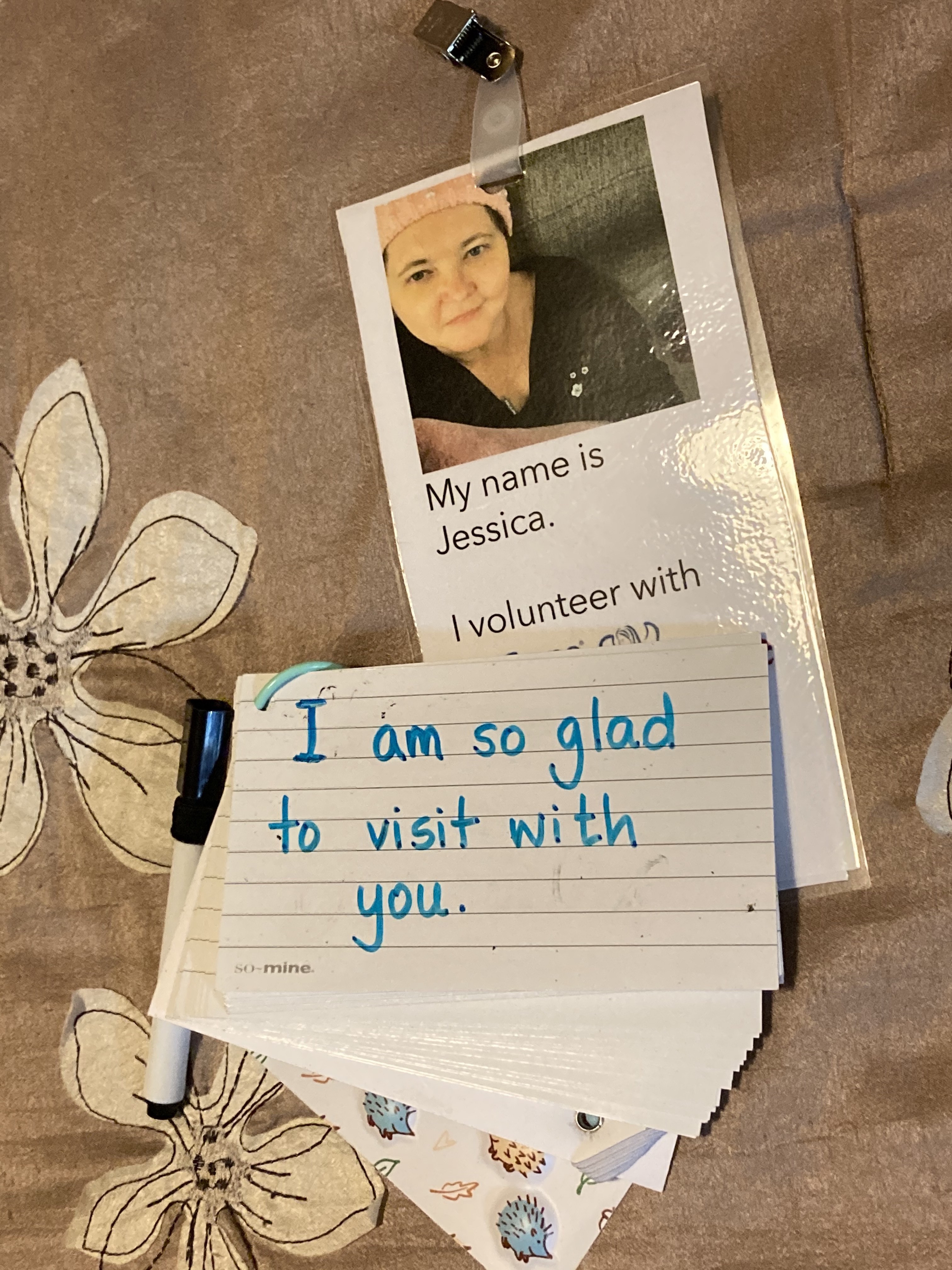
I held up my i.d. badge (which also has my photo), and pointed to my name while I said it. Then I showed her a card on which I had written, “I am so glad to visit with you.” That’s something I have expressed (spoken and with this card) every time I have come.
Next I wrote, “Your leg is tangled?” I pointed at each word and read it to her twice. I showed her a card that said, “Do you have pain?” She nodded and gestured to her right leg under a blanket. The blanket was not twisted though, and nothing about her leg or foot appeared out of the ordinary (no discoloration, no swelling).
So I wrote, “Would you like your bed more up or more down?” She said yes, talked me through how to use the gizmo, and reported that it was better. I sat back down.
She said, “I’m sorry.“
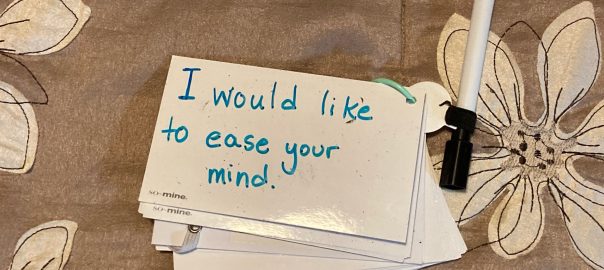
I wrote and spoke, “I would like to ease your mind.“
She said, “Oh, thank you.”
Everything about her relaxed — her face, her posture, how she held her blanket. She lay back, and was asleep again before I wrote anything else. I sat with her awhile longer in case she roused again, but her breathing was regular and calm.
In turning it over in my mind, I feel like the conversation unfolded with statements and questions that were responsive to her even without understanding. That made them helpful to me also.
Still learning, how to listen, what to say, and why.
Before my dad was officially diagnosed with ALS, the working theory for his abrupt weight loss was digestive: in short, he wasn’t eating enough calories. This explanation was elevated in the assessment process because one of the words he used to describe how he felt was “nauseous.” It wasn’t until I was with him over several meal attempts that I realized we needed to examine that word more closely.
To me, nauseous meant an unsettled feeling in the stomach and a pronounced urgency to throw up; I associated it with a franticness of wanting to find some where to vomit, not on myself. But my dad wasn’t doing that — he would say he was nauseous and then lie down. I believed him that his body was giving him cues and that he was acting on those with personal expertise, and I wondered if there might be other words that better matched his experience. While he rested, I did a search on synonyms.
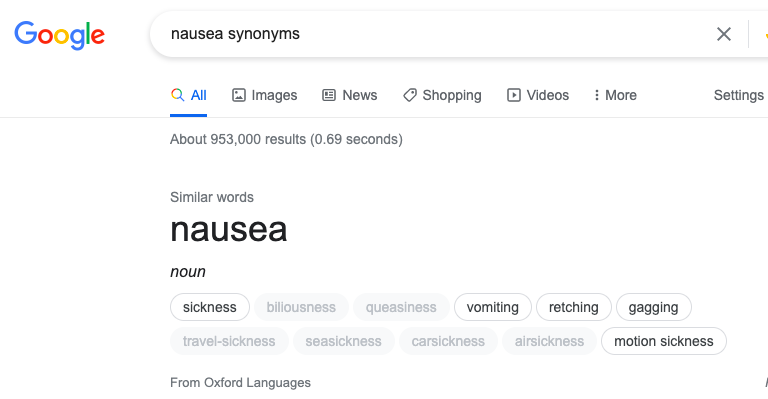
Screenshot of a Google search for “nausea synonyms” identified: sickness, biliousness, queasiness, vomiting, retching, gagging, travel-sickness, seasickness, carsickness, airsickness, motion sickness. These were said to be “From Oxford Languages”
The two that jumped out at me were biliousness and queasiness; ironically, since these were both in a paler font. Others were associated with specific circumstances (various kinds of travel or motion sickness), which also gave us the idea of making comparisons between how he felt at that time in references to past situations of being unwell.
When we changed the conversation to add specificity to his wording and detailed comparison and lack of similarity from other circumstances, it started to change the direction of our thinking. Unfortunately, it took a little longer for his familiar medical team. They weren’t ready to rule out digestive concerns, and it took my dad’s sense of himself + his understanding of his rate of change to compel a different team into re-examining the available evidence. I also believe that another factor was the urgency expressed by my cousin to the ER doctor in the hall, making it profanely clear that her background as a nurse and knowing my dad was a clanging alarm bell that she intended to have heard.
I believe that the words we use matter. What I don’t know is whichwords most accurately convey information which can be translated when it is needed most. Sometimes words chosen can light the path to a solution, and sometimes it is a misdirect that increases pain and suffering.
Regina Fink, RN, PhD, AOCN has studied pain assessment, and has compiled the WILDA approach:
Words to describe pain
Intensity (0 to 10)
Location
Duration
Aggravating and Alleviating
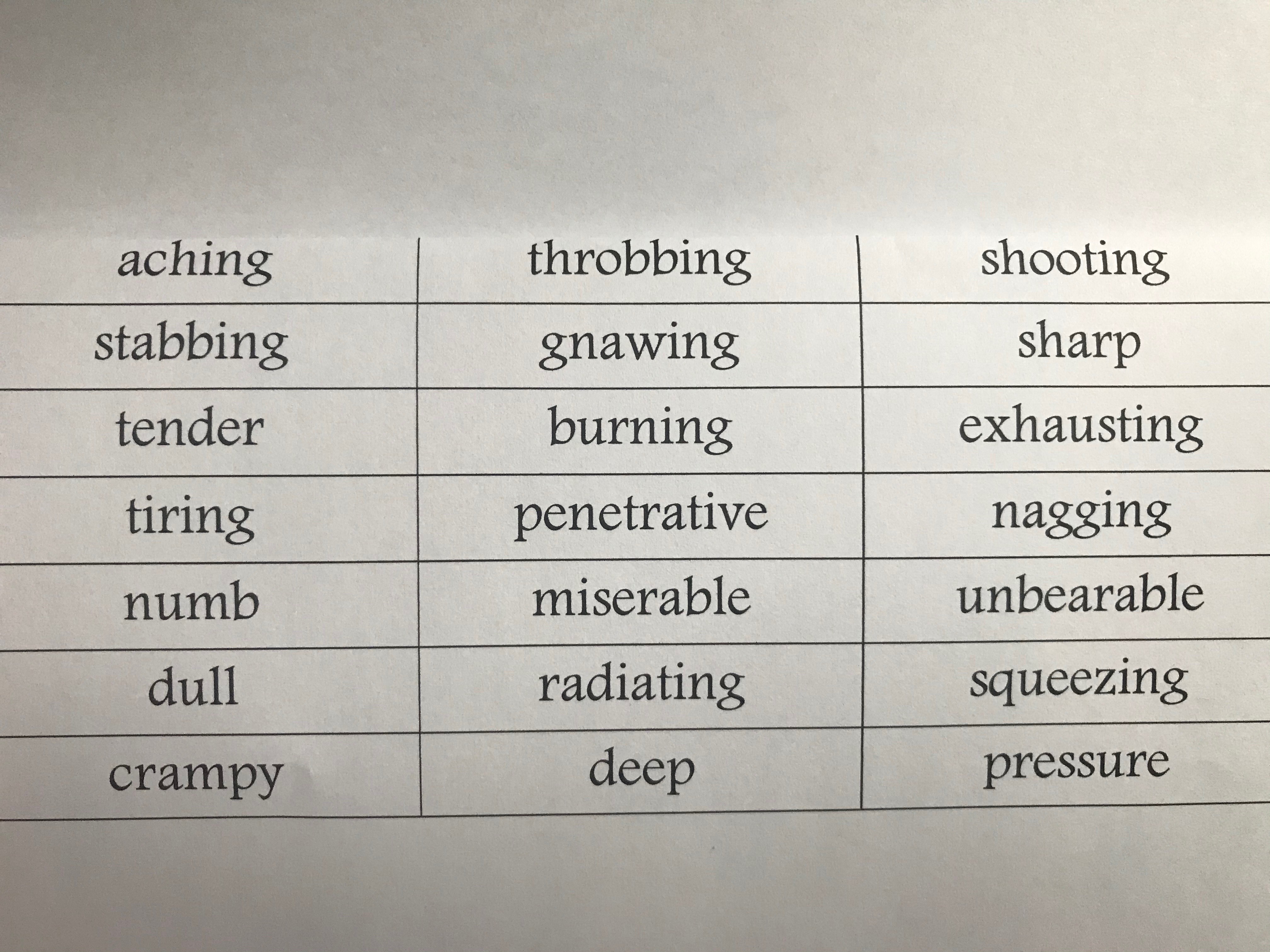
Dr. Fink provides a detailed and helpful analysis of each component of the in the 2000 Baylor University Medical Center Proceedings titled, Pain assessment: the cornerstone to optimal pain management. It is well worth reading and I highly recommend it. I have strong opinions about the use of intensity ranges as the sole quantifier of pain/concern which I have gone into detail about elsewhere. For my purpose presently, I am focusing on the first section she discussed relative to words to describe pain — she goes on to explain how these lend insight in ways that are associated with nerves, muscles, and organs:
Word bank of terms to describe physical pain which includes descriptions of neuropathic discomfort, somatic, and visceral. Each category have different ways they locate and behave in the body — such as specific to one spot or across a general area.
In terms of health literacy, I feel like these are the seeds of a glossary we should be talking about, at a minimum, when relaying our experiences of pain to medical teams. These also are critical to be teaching our kids relationships with their sensations so that they are able to interact with confidence and autonomy. A shared vocabulary is critical for a culture of informed consent.
In talking with a dear friend about the WILDA approach, she asked two incredibly important questions:
What about non-physical pain? The WILDA vocabulary do not apply well to mental, emotional, social or spiritual/existential pain. We agree that it is misguided to conceptualize these as exclusive or can be distinguished from one another.
How do we move beyond a comparison of pain against NO-pain? If zero discomfort is the standard of ‘normal,’ both she and I are immediately out of the conversation because that does not happen for either of us.
I don’t have an answer to these questions even just for myself, but I do know that I benefit from conversations about it and that sometimes having a starting place to bounce off of helps advance the cause.
A book that has been helpful as a parent is Maria Lamia, PhD’s Understanding MYSELF: A kid’s guide to intense emotions and strong feelings (2011).
Dr. Lamia’s review gives broad descriptions of emotional landscapes and provides key words that may be associated with these. Each chapter includes information in straightforward language, first-person kid quotes, a short survey of self-evaluation, resources for building resilience, and some research-based science. There’s part of me that experiences my pained and suffering Self aschildlike…that I do best in understanding, relating and creating spaces for healing when I can hold myself gently in that mindset.
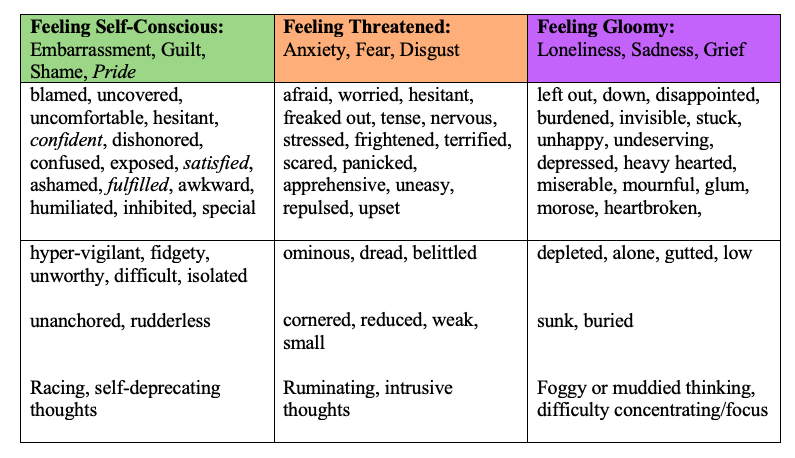
I reviewed Dr. Lamia’s vocabulary for the areas of Feeling Self-Conscious (which includes embarrassment, guilt, shame, and pride), Feeling Threatened (as with anxiety, fear, and disgust), and Feeling Gloomy (loneliness, sadness, and grief).
Note: I kept the terms for Pride in the table, but I tend to associate that as a positive and I am not sure how that would correspond to medical/mental health teams at least in the same way as the other feelings and emotions.
A table of vocabulary grouped by Mary C. Lamia (2011) categories in columns of Feeling Self-Conscious, Feeling Threatened, and Feeling Gloomy. The second row includes additional words from my own experience with feelings, social implications, and thought energy flows I associate with each column.
With my kids, I can just turn to the main chapter grouping and have them review the words — typically, they find that there are a few that ‘jump out at them’ almost as if they were written in a special font at that moment. Now that they are teens, we can talk more about the nature of their thinking — are thoughts like ping-pong balls, bouncing out of control? How about circling around or spiraling outward from a central, negative idea? Maybe just stuck and unmoving?
I say this is something I do with my kids, which it is, but it is as much a process I am trying to learn myself as it is something I hope to impart as a parent.
Two photos of the same tree. On the left, it appears round and full. On the right, it is evident that the trunk and crown are actually U-shaped with an enormous gap in the leaves for where it has been pruned back for power lines.
So that’s where I am with this, fully aware that this is not a whole picture.
I do not yet have vocabulary for really any social or spiritual/existential pain — although I suspect there is some overlap within aching loss and/or feelings of being outside of a higher order of belonging.
I also know that there are cultural differences in the experience of word meaning particularly as it relates to co-constructed understanding as with exchanges of information. As one example, being white may have had an influence on my cousin’s use of profanity as being heard as emphatic and passionate rather than with implicit biases of being unsophisticated, threatening, or disrespectful. Conversations among speakers of the same primary language undoubtedly go more smoothly than when there is a translation involved — particularly when some languages may not share common meaning in expression or tone. The very real risk is informed consent may not be achieved, and in medical-health situations that rapidly becomes dangerous.
I want to do better: I want to learn more. I want this to be just a beginning.
I originally posted this on social media 5 May 2011, which was just before my kidney transplant surgery. I was on outpatient hemodialysis three times a week, and I knew my life was on the threshold of unimaginable changes. I’m still reflecting on what I know now compared to then, so this is just giving acknowledgement to that time.
“There’s no question that I’m in a bit of a headspace about how to process/navigate it all, and I’m not altogether comfortable with the role of my ego in all of this. I will say though, I have enjoyed this process/experience infinitely more than judging myself on whether or not I had accomplished enough any particular day (go figure), and have truly valued this consideration of what is truly important to me. There will always be laundry, or books about how to parent, or something I haven’t done yet for my husband/children/job/family/dear friends, etc., etc., etc. But really, most of that is just the superficial distractions on top of the real work of living.
To Be
1. Breathe. I am here, now. I am alive, now. I only have moments to live (specifically, this moment).
2. Nurture an open heart. I believe this is my best/only hope for being free.
3. Make deliberate choices which support my values. I feel like I’ve come upon a 3-part rule which seems to me to be perfectly true: (1) Decide to do that which will cause the least stress/pain later, (2) When in doubt, if only because it is the easiest remember: tell the truth, (3) Make the choice which is most consistent with what I want my best self to be. I have yet to find a situation where these don’t apply.
4. Pay attention. Combined with #1 or #2, I feel well aligned with a “Life moves pretty fast. If you don’t stop and look around once in a while, you could miss it.” (Ferris Bueller, 1986). Ironically though, combined with #3 this is probably one of my strongest coping strategies. Despite how it may appear, I do not consider myself to be an especially “optimistic” person. I make very deliberate choices about what I’m going to pay attention to (how incredibly awesome and amazing the majority of my life is), and what I feel is less important in the grand scheme of my values.
5. Speak, listen, and be with silence. Not necessarily in that order.
6. Practice 1- 5 often. None of these are achievable without cultivating them on purpose. They may be simple, but they are not easy.
At some point it occurred to me that, as part of being a fan of balance, yin and yang, something/nothing, Shakespeare, I also have a solid list of what I think Life ISN’T about.
Not To Be
1. Life is not a chicken. I don’t choose which parts I like and which parts I leave at the bottom of the bucket. It’s all life. Whether you want to take a, “no waves, just ocean” view or a Paul’s letter to Corinthians, Chapter 12:12-27 (if you happen to take a religious stance), or a “Nothing human is alien to me” (Terence) approach. My life may, at times, seem grossly unnatural, or marked by pain or despair, or any number of descriptions that are not appealing or pleasant. But denying or railing against what clearly is seems to me to be a waste of what time and energy I do have. Applying this outwardly, I find that this belief joins with “nurture an open heart” and how I hope to receive other people’s experiences without judgment whenever possible. It is not for me to say what is “right” of/for others, there is no benefit in doing so, and it ultimately pains me to be divided from others by those who would cultivate fear or hatred of difference.
2. Life is not a scoreboard. I should do things because they reflect deliberate choices aligned with my values, and that is its own reward.
3. Life is for living, not lists. No matter how I try to craft the perfect summary of what I believe, or compose a sincere, ‘Everything I need to know I learned on Facebook,” poster, it would be better for me to log off and get back to the real work of living. A segment of a Warren Miller documentary profiling paraplegic extreme skiers, one had written “Die Living” on his sit ski and I can’t help but feel that he’s right. Oh, Life: What an ocean of experience!