This expression was popularized by Mark Twain, which appeals to me on many levels; however, there are inconclusive reviews on how it may have originated before his use 1907. I undoubtedly heard it first from the tv show, “West Wing” and all of this is to say that I am entrenched in thinking about what do I know, how do I know it, and variations of expressing it. I wrote last about numbers and that’s still where my head is at — the alluring quality of having objective, quantifiable values which serve to communicate in a tidy way.
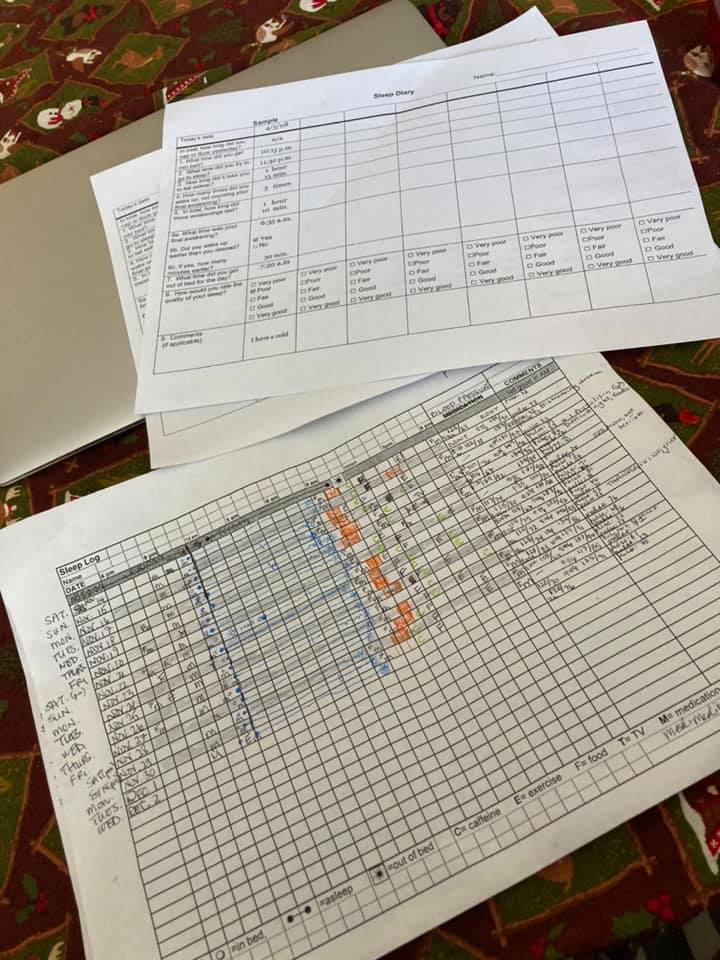
In November of 2020, I decided I was not prepared to continue hating my sleep experience (horrific dreams) and worrying about constant fatigue. Although I have reported these concerns to many physicians over the years, for some reason it landed differently this time and that lead to my meeting with a Sleep Specialist and, separately, a Cognitive Behavior Therapist with specific focus on Insomnia. They both wanted data tracking, and in different formats. I was/am willing to do this because it is within my capacity and I do not want to resign myself to feeling this way about 1/3 of my on-going life in perpetuity.
The thing is:
- it is itself exhausting to document all of this
- much of measures like these are poorly defined/constructed
- I am not unfamiliar or averse to data collection; however, I don’t know how to do this better.
- How do people who have even less energy or experience with analytic tools participate in this meaningfully
- If they aren’t, what function does perpetuating these practices serve?
Documentation Weariness
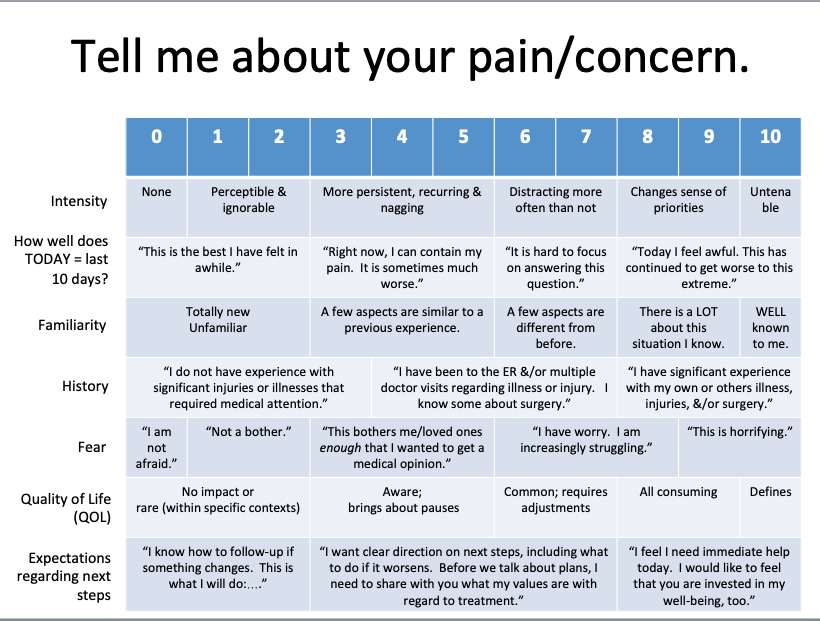
If you’ve never been asked to characterize part of your experience of being you with a number or code it may be hard to explain WHY it can be an existential conflict. Or if you are in a mindset of “I would do anything to get back to normal”, exercises like this seductively feel like breadcrumbs on the path to status quo ante. I mean, maybe they ARE. Maybe both things are true: it is difficult to remember your own humanity as separate from the notes you make about yourself, AND this information is helpful towards living the human life you most want for yourself.
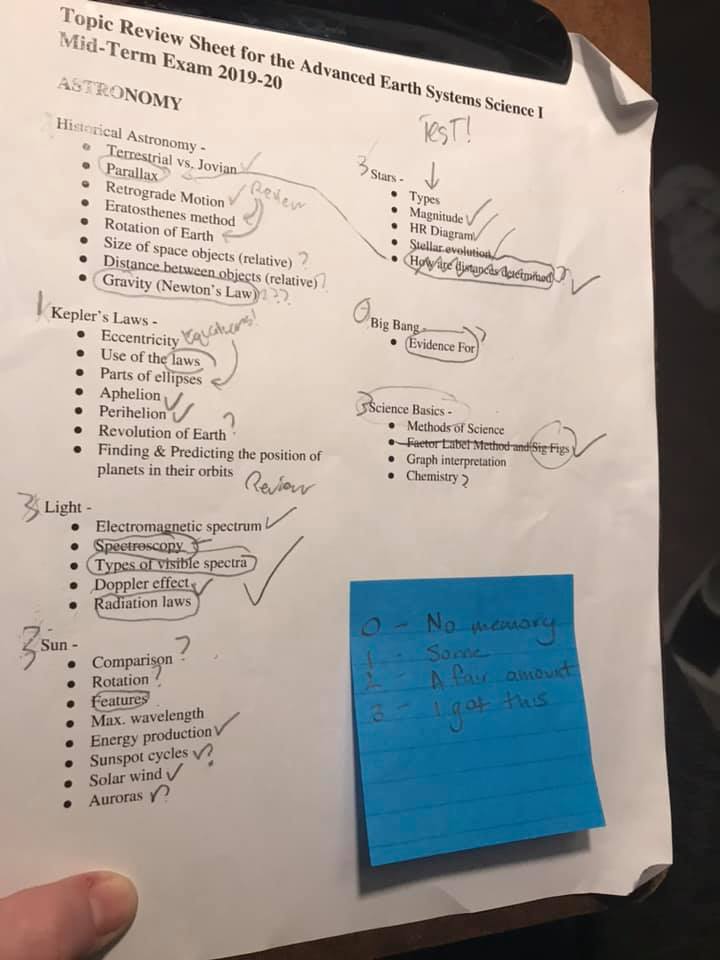
One of the successful uses of a rubric that I developed was with my son to support his ability to prioritize his study efforts was to review the topics and focus on what he remembered the least. Ironically, I would characterize my recollection of all of this at a 1 or a 0 if it had not been for the photo (shout out to visual cues). This was easy to use, and felt rewarding at being able to transition low rated topics to more solid recall.
Definitions and structure
Often there is a balance being struck between ease of scoring (which is different than ‘interpretation’), and how much information is actually being relayed. With the sleep diary, I am asked to characterize my night along a five-point range from “Very Poor” to “Very Good” and I have no idea how to regard that. I keep telling myself that I am empowered to come up with a rule and then just apply it consistently. But I know that I have two distinct sleep goals: (1) to feel rested with quality and quantity of sleep, and, separately, (2) to not be horrified by absurd dreams which leaves me anxious about entering sleep. There’s only one column per day, one allocation for each day and I genuinely do not want to ADD anything more to the stuff I am already writing down. It may be that I am too close to do this personally for myself.
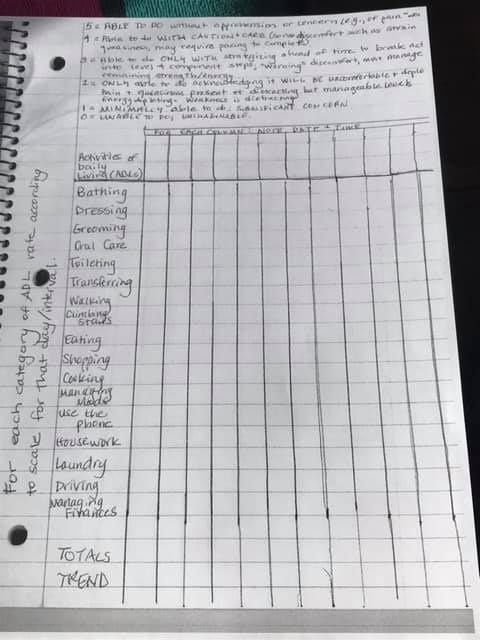
When my Dad was declared to have an aggressive form of Amyotrophic Lateral Sclerosis (ALS), he became the 12th person I had directly interacted with to have an ALS diagnosis. I had on-hand multiple scales for characterizing ability/decline — which I used in assessment reports specific to communication complications. In my interactions with my Dad though, I realized some important distinctions were necessary.
Working with him, we developed a scale to be more refined:
5 = ABLE TO DO without apprehension or concern (e.g., or pain, weakness, etc.)
4 = Able to do WITH CAUTION + CARE (some discomfort such as strain or queasiness anticipated, may require pacing to complete)
3 = Able to do ONLY WITH STRATEGIZING ahead of time to break acts into Level 4 component steps; “warning” discomfort, must manage remaining strength/energy
2 = ONLY able to do acknowledging it WILL BE uncomfortable and depleting. Pain and queasiness distracting but manageable. Energy depleting. Weakness is distracting.
1 = MINIMALLY able to do: SIGNIFICANT CONCERN
0 = UNABLE to do; UNIMAGINABLE
I do not presently remember how our scale was received by his medical team…in many ways, I don’t care. In this method it became a useful tool for he and I to plan effectively and it served to clarify for him that progressive decline meant it was not going to get better. His previous life experience, pronouncedly different from my own, was that the strength of his will + optimism powered him through illness or injury. That is my caveat for wanting tools such as these to be “rewarding”: sometimes the trend they reveal is not one that would typically be welcomed or celebrated.
As I learn better, I aim to do better.
I am writing this out in hopes that it can stop bouncing around my head. I know I am in a hole with this and I haven’t been fully honest about the documentation that’s actually gotten me here-here. I’m supposed to be writing down my feelings as distinct from my thoughts and the internal resistance I feel towards this task is palpable to me.
I haven’t landed on WHY I find this so different compared to characterizations based on number values and rating scales. Each time I sit down to do it, my mind goes blank: a grey landscape. Every additional noise in my environment commands my attention instead, and also the laundry, or dishes, or hanging out with my family…
Nagging at the back of my head though is that I value being a Good Patient. I do not want to return to my physician without having done this. She needs me to do this so that we can advance what I value as progress towards my goals. (sigh)
Who is this helping?
In “Wounded Storyteller,” author Arthur Frank details how medical practice has evolved from localized expertise within communities who interacted with their neighbors, to industrialized depersonalized methods in which essentially strangers translate symptoms into billable codes. Being able to indicate that I gradually characterized my sleep experience from “Very Poor” to “Fair” to “Good” would be evidence; proof of benefit. I get that. As a speech-language pathologist, I have done that and, should I go back there someday, I may need to again.
Right here right now though, I have concerns that that this business of being tidy is more problematic than it is helpful. I do want to honor what physicians and medical teams know and participate in the work of my well-being. I do not want that to include shame that I did not do enough or clearly. I absolutely do not want these kinds of activities to be used against patients as proof of non-compliance or failure to follow physician’s orders.
Back when I was on dialysis, I was told that my insurance company might track my schedule to make sure that I came to dialyze when I was supposed to and stayed the full duration indicated by the discrepancy from my dry weight. If there was a concern that I wasn’t coming or left early, the insurance company might decide not to reimburse the expenses. I do not know if this was true. I am a rule-follower by nature so I absolutely was not going to miss any sessions. I was also already terrified about bankrupting my family with how expensive I was to keep alive, so I did not need a documentation/compliance scare story to add to the mix.
I am confident that there are ways to monitor and inform treatment plans. I believe that documentation is a critical element of health care…And.
“What gets us into trouble is not what we don’t know. It’s what we know for sure that just ain’t so.” — Mark Twain
End blip.