Before my dad was officially diagnosed with ALS, the working theory for his abrupt weight loss was digestive: in short, he wasn’t eating enough calories. This explanation was elevated in the assessment process because one of the words he used to describe how he felt was “nauseous.” It wasn’t until I was with him over several meal attempts that I realized we needed to examine that word more closely.
To me, nauseous meant an unsettled feeling in the stomach and a pronounced urgency to throw up; I associated it with a franticness of wanting to find some where to vomit, not on myself. But my dad wasn’t doing that — he would say he was nauseous and then lie down. I believed him that his body was giving him cues and that he was acting on those with personal expertise, and I wondered if there might be other words that better matched his experience. While he rested, I did a search on synonyms.
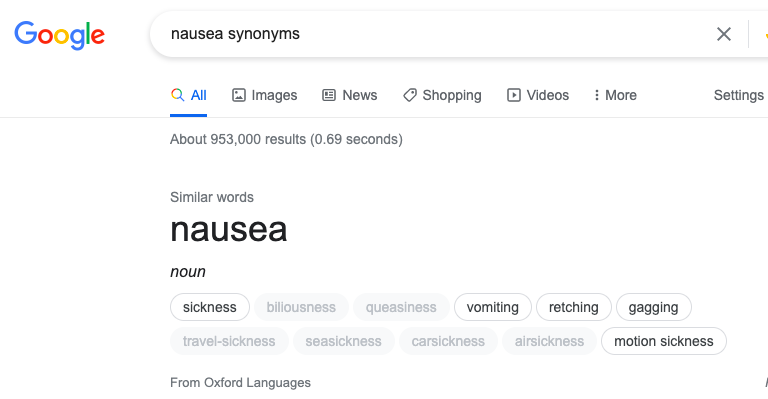
The two that jumped out at me were biliousness and queasiness; ironically, since these were both in a paler font. Others were associated with specific circumstances (various kinds of travel or motion sickness), which also gave us the idea of making comparisons between how he felt at that time in references to past situations of being unwell.
When we changed the conversation to add specificity to his wording and detailed comparison and lack of similarity from other circumstances, it started to change the direction of our thinking. Unfortunately, it took a little longer for his familiar medical team. They weren’t ready to rule out digestive concerns, and it took my dad’s sense of himself + his understanding of his rate of change to compel a different team into re-examining the available evidence. I also believe that another factor was the urgency expressed by my cousin to the ER doctor in the hall, making it profanely clear that her background as a nurse and knowing my dad was a clanging alarm bell that she intended to have heard.
I believe that the words we use matter. What I don’t know is which words most accurately convey information which can be translated when it is needed most. Sometimes words chosen can light the path to a solution, and sometimes it is a misdirect that increases pain and suffering.
Regina Fink, RN, PhD, AOCN has studied pain assessment, and has compiled the WILDA approach:
- Words to describe pain
- Intensity (0 to 10)
- Location
- Duration
- Aggravating and Alleviating
Dr. Fink provides a detailed and helpful analysis of each component of the in the 2000 Baylor University Medical Center Proceedings titled, Pain assessment: the cornerstone to optimal pain management. It is well worth reading and I highly recommend it. I have strong opinions about the use of intensity ranges as the sole quantifier of pain/concern which I have gone into detail about elsewhere. For my purpose presently, I am focusing on the first section she discussed relative to words to describe pain — she goes on to explain how these lend insight in ways that are associated with nerves, muscles, and organs:
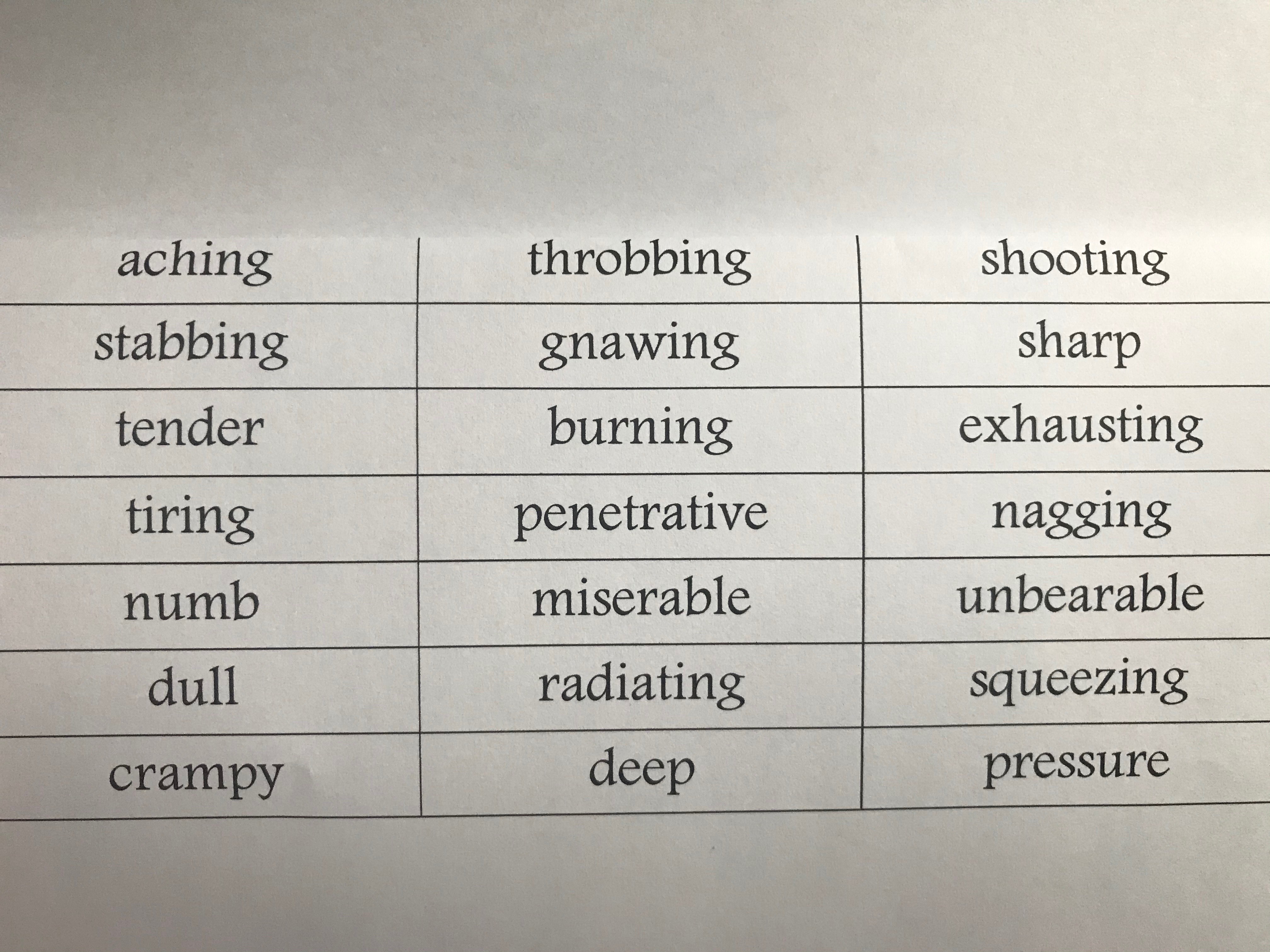
In terms of health literacy, I feel like these are the seeds of a glossary we should be talking about, at a minimum, when relaying our experiences of pain to medical teams. These also are critical to be teaching our kids relationships with their sensations so that they are able to interact with confidence and autonomy. A shared vocabulary is critical for a culture of informed consent.
In talking with a dear friend about the WILDA approach, she asked two incredibly important questions:
- What about non-physical pain? The WILDA vocabulary do not apply well to mental, emotional, social or spiritual/existential pain. We agree that it is misguided to conceptualize these as exclusive or can be distinguished from one another.
- How do we move beyond a comparison of pain against NO-pain? If zero discomfort is the standard of ‘normal,’ both she and I are immediately out of the conversation because that does not happen for either of us.
I don’t have an answer to these questions even just for myself, but I do know that I benefit from conversations about it and that sometimes having a starting place to bounce off of helps advance the cause.
A book that has been helpful as a parent is Maria Lamia, PhD’s Understanding MYSELF: A kid’s guide to intense emotions and strong feelings (2011).
Dr. Lamia’s review gives broad descriptions of emotional landscapes and provides key words that may be associated with these. Each chapter includes information in straightforward language, first-person kid quotes, a short survey of self-evaluation, resources for building resilience, and some research-based science. There’s part of me that experiences my pained and suffering Self as childlike…that I do best in understanding, relating and creating spaces for healing when I can hold myself gently in that mindset.
I reviewed Dr. Lamia’s vocabulary for the areas of Feeling Self-Conscious (which includes embarrassment, guilt, shame, and pride), Feeling Threatened (as with anxiety, fear, and disgust), and Feeling Gloomy (loneliness, sadness, and grief).
Note: I kept the terms for Pride in the table, but I tend to associate that as a positive and I am not sure how that would correspond to medical/mental health teams at least in the same way as the other feelings and emotions.
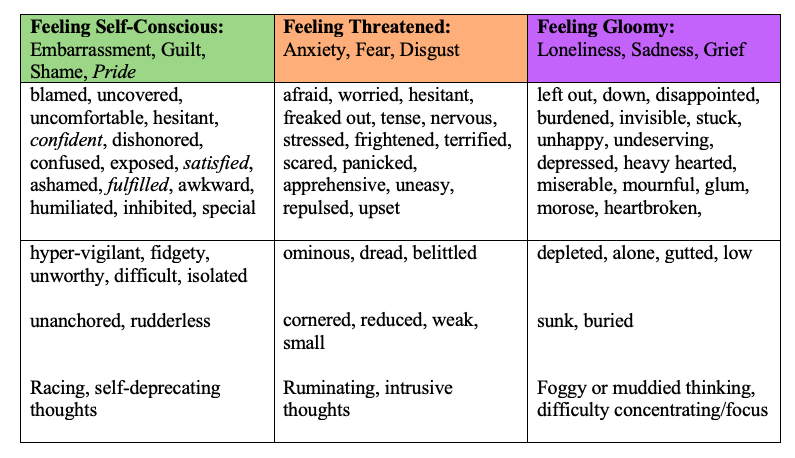
With my kids, I can just turn to the main chapter grouping and have them review the words — typically, they find that there are a few that ‘jump out at them’ almost as if they were written in a special font at that moment. Now that they are teens, we can talk more about the nature of their thinking — are thoughts like ping-pong balls, bouncing out of control? How about circling around or spiraling outward from a central, negative idea? Maybe just stuck and unmoving?
I say this is something I do with my kids, which it is, but it is as much a process I am trying to learn myself as it is something I hope to impart as a parent.

So that’s where I am with this, fully aware that this is not a whole picture.
I do not yet have vocabulary for really any social or spiritual/existential pain — although I suspect there is some overlap within aching loss and/or feelings of being outside of a higher order of belonging.
I also know that there are cultural differences in the experience of word meaning particularly as it relates to co-constructed understanding as with exchanges of information. As one example, being white may have had an influence on my cousin’s use of profanity as being heard as emphatic and passionate rather than with implicit biases of being unsophisticated, threatening, or disrespectful. Conversations among speakers of the same primary language undoubtedly go more smoothly than when there is a translation involved — particularly when some languages may not share common meaning in expression or tone. The very real risk is informed consent may not be achieved, and in medical-health situations that rapidly becomes dangerous.
I want to do better: I want to learn more. I want this to be just a beginning.
[End blip.]