For awhile now, I have been working to refine my sense of physical and emotional suffering, which I termed globally as pain/concern. More recently I have been trying to wrap my thinking around a different combination of physical and mental complications. My assessment of whether or not I can do something, am successfully doing it or need to adjust immediately, or believe I cannot do it and will not even try includes: anticipating pain or task failure, in-the-moment pain or mistakes, and backlash either as regret, ache, or a mess that shows up later. It’s a heady mix of questioning strength and confidence.

What I remember most clearly about the moments immediately after when I had destroyed our table, was that it had not in any way occurred to me that I couldn’t do this on my own. I had retrieved the umbrella from the shed, carried it across the yard + up the porch steps, held it over the height of the table to position it in the center…
I had done this before — it was not a new task to me although it was typically only once in Spring install and one-time removal in Fall. I don’t think I knew the table was glass. It never occurred to me that it could completely crumble into a gazillion sharp edged pieces…
Also, I was in somewhat of a hurry. Food was in some stage of being prepared, the 8-year-old twins were ready to eat. I couldn’t let them anywhere near this. I didn’t want anyone else to have to clean up this catastrophe. I kept imagining bloody footprints from yard creatures getting cut by my gross err in judgment.
Worse still, I was not physically capable of cleaning it all up. I became dehydrated and light-headed, the glass was too heavy, the sunshine blazing. I was so deeply sad that I had to give it over to my husband. It all felt awful.

In the moment, I did not see the fall at all. I know I witnessed it at a subconscious level because it was returned to me in dreams later. Had I noticed the step, I am sure I could have been both physically strong and entirely confident = successfully completed the act without injury. But that really does not matter because that’s not at all what happened.
Sitting on my couch right now, I cringe and fix my jaw at the memory of it even still. My sense that I will see the potential problems feels pretty unreliable. Where do strength and confidence go?
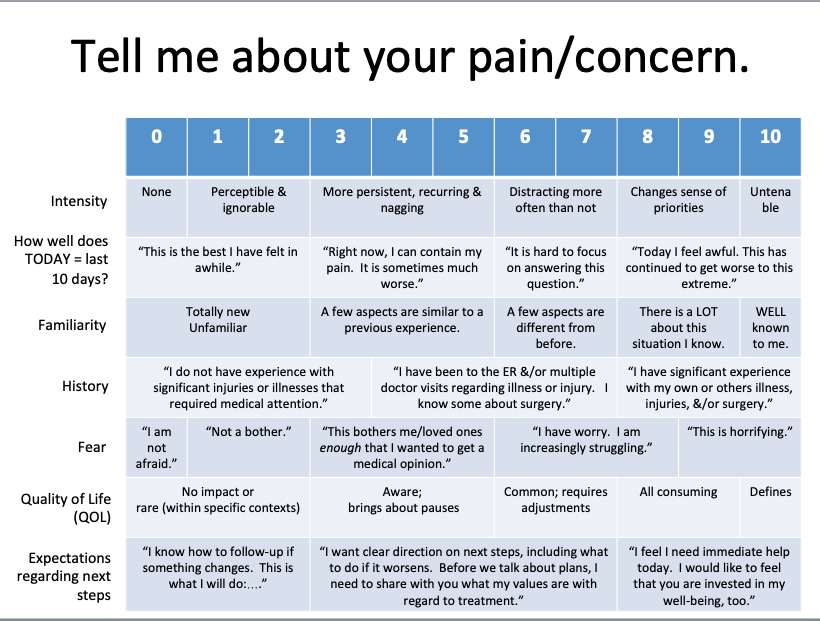
If these kinds of categories were to get added to the Tell Me About Your Pain/Concern, how would I quantify anticipatory pain/worry? I have used the terms “ominous” and “dread” to physicians and physical therapists; as in, “I have an ominous sense that I am going to have severe heart burn from my potassium supplements, and I have to remind myself to relax or it is more likely to get stuck in the tension of my throat.” Or, “I know I am carrying myself very cautiously on walks because of dread that I may stumble.” I know that this is primarily a mental-emotional issue, and it matters because it directly influences how I act in the world even for the most basic activities of day-to-day living.
In 2019 when my Dad was in rapid progressive decline with ALS, I noticed trends which were both physical and mental-emotional in him (it’s easier to see such matters in other people than I tend to in myself). There was almost nothing he could do with complete autonomy and no modifications; but sometimes it was my sense that he answered according to what he wished were the case or based on how he had done the last time he’d tried even if that was awhile ago. Together we came up with a more representative set of characterizations:
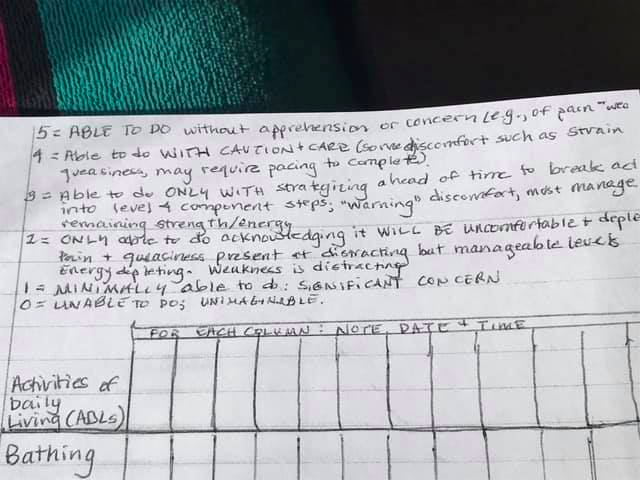
5 = ABLE TO DO without apprehension or concern (e.g., not afraid of pain, falling, etc.): If he was already seated or lying down, he could use his telephone for brief calls.
4 = Able to do WITH CAUTION and CARE (that is, some discomfort likely such as strain or queasiness, may require pacing or preparation to complete). He could complete oral care tasks from a bathroom seat. He could consume protein drinks by straw. He had prepared his tax filing documents just before he started struggling more prominently, so in that sense he was well positioned with his finances.
3 = Able to do ONLY with strategizing ahead of time to break task into level 4 component steps; “warning” discomfort expected; must manage remaining strength and energy. In terms of managing medications with respect to dosages and times, this was probably at a 5; however, actually taking pills required numerous steps by others (assembling, crushing to powder, mixing in with applesauce or pudding), and also himself (remembering safe swallow techniques, pacing energy consumption for sitting up, etc.)
2 = ONLY able to do acknowledging IT WILL BE UNCOMFORTABLE + depleting. Pain + queasiness present at distracting but manageable levels. Energy depleting. Weakness is distracting. Walking with a physical therapist was dreaded even when at an emotional level he valued the concept; transferring into and out of the wheelchair.
1 = MINIMALLY able to do; SIGNIFICANT CONCERN: Toileting was a tremendous issue.
0 = UNABLE to do; UNIMAGINABLE: the idea of walking down more than 3 steps, doing laundry, and driving were all extremely complicated physically and cognitively, all bore very high probability for serious injury to the point it really wasn’t worth debating.
There are a number of standard ADL lists that I did not include in this because they weren’t relevant to my Dad’s life at that time — cooking and housework were not part of his daily life.
As I reflect on all of this now, I can see how these rankings incorporate both
- the physical demands of the task, which includes capacity, strength, stamina, persistence and
- a sensibility of prognosis: based on (recent) past experiences, what confidence do I have that I can do this successfully.
Said differently, how a person gauges across both of these that they can start, do, and complete something without needing someone else, and without having an accident which makes a bigger problem as either a mess or an added injury.
For as much as I dislike the anxiety + self-doubt of anticipating pain or task failure ahead of an event, the other end of this gamut is achy backlash, regret hangover, or aftershock. It is nerve pain that feels EXACTLY like a bee sting when I am brushing my teeth at the end of the night, knowing with certainty that I have not been stung but rather this is a residual complaint from an aggravation I did not notice at all in the moment it occurred. It is waking up the next day unable to turn to the left after carrying heavy groceries upstairs (maybe that’s what it was?). It is overwhelming guilt that maybe I will not go sledding with my kids next time because this time many muscles and joints hurt so, so badly by dinnertime. This may be the most debilitating of pain/concern because it lands so deeply in my ocean of shame. It is in these moments where my sense of myself — my personal metric of strength and confidence — is most challenged. Activities that do not come with a delayed pain/concern do not register in my memory. As a result, they contribute a much quieter impression of what I can do successfully.
As I read over all of this, I am reminded that my attitude about developing a Tell Me About Your Pain/Concern scale has always been as a tool for communication, patient advocacy, and health literacy. I’m not developing a screening measure or billing code where scaled numbers are calculated vertically to a singular number. What I really hope for all of this is to promote a broad-based framework towards productive conversations and those get individualized (more narrow) with the follow-up questions. With this in mind, characterizations about fear and quality of life could be immediately linked with further investigation of the role of strength and confidence.
It also validates making an explicit practice of “I did that” recognition — making sure that these become part of my history of me. This could be paired with explicit practice in low-stakes tasks: identifying when I have moments of doubt, and exploring those experiences in ways that I can readily find the boundaries of my strength and confidence. I may always have <5 ratings within my activities of daily living capabilities — may those be opportunities to build, broaden, adapt, and share with my medical/health care team.
End blip.
p.s. I did that.