Very often this online journal has been a place for me to explore my thoughts and experiences. I keep it ‘public’ because I believe that sharing our stories with one another allows us to learn better and more collectively.
Recently I realized I had quite a few photographs that may serve to illustrate ways to interact with elders.
For those unfamiliar, “Spoonie” is a tangible metaphor for those ailments which may not be ‘visible’ but which absolutely impact/define life. The idea was first introduced by a woman who has Lupus, and she used a quantity of spoons to represent energy throughout the day.
To a friend who did not have Lupus, getting up, picking out an outfit, taking a shower, getting dressed, doing hair and make up, eating breakfast and heading to work might just be one spoons worth of energy titled “starting the day.”
For a person with Lupus or motor-coordination differences, depression/anxiety/apathy, or any number of other challenges, just getting out of bed might ‘cost’ an entire spoon. With 11 left to get through the entire rest of the day.
Last night I realized that the story is pretty easy to imagine, but incomplete. Not all of my spoons are equivalent. Some situations I have superpower spoons that get me through: I cope with medical procedures and manage my emotions and energy very well. I do not cope with uncertainty or self-doubt well, and those spoons can disappear into a a very sad fog.
Last night, I was disappointed in myself for being tired, and remembered times when the kids were little that I could pull from a well of will power to get through. Then it struck me: when the kids were little, I was *younger*, and a lot had not happened yet that contributes to my collection of available spoon cache now.
I forgave myself for being tired. I forgave myself for wishing I had a different set of spoons/circumstances. It’s okay that sometimes I am in a sad fog about that: It is sad, and it is foggy.
I was reminded, too, that I have skills in readjustment. So, right here, right now: I surrender to the illusion of control. My spoons are mine. My body, my life, my feelings are mine.
For want of a functioning kidney, my immune system is suppressed. In the absence of an intact immune system, I am prone to infections. Having more than one infection in a short amount of time (or the same infection persists beyond an initial treatment), and more than one antibiotic is used, my gut biome developed Clostridium difficile Toxin B gene, and Stl c-diff Toxin A&B — commonly known as “c-diff.”
I’ve heard this diagnosis applied in my general vicinity before (in 2009 and 2018), so it didn’t ricochet off my mind as unimaginable. That phenomenon does happen sometimes — having no prior knowledge of something makes it harder to reconcile — just not this time. What was new was every single medical person I spoke to asked if I’d had it before.
I’m pretty sure that’s code for: “If this happens once, it is more likely to happen again.“
And: “If you have been through this symptom profile, you know what is happening.“
Recognizing and deciphering unusual language and codes is part of the experience of illness, not unique to chronic or life-impacting ones. Who remembers the first time they fully connected all of the terms and slang of throwing up with the act and result of vomiting? That labeling probably is not recognized — but it all becomes part of the experience known and understood in the mind-body.
What would I do differently? None of it. The functioning kidney, suppressed immune system, treating adverse conditions as they come (even with risks) = steps on the path adjacent to being with my loved ones. I added this experience to the medical history I keep in my purse. I made other revisions, too.
A table of my relationship to pain/worry on a 0 to 10 scale which defines increments of intensity (where 0 = None, and 10 = Untenable), fear (ranges from “I am not afraid” to “This is horrifying”), quality of life (as “No impact or rare” [on QOL] to “Defines” [QOL]), and My Lived Experiences with examples of personal discomfort and/or duress.
These already take into account my familiarity (I’m not as afraid or limited by physical and emotional pains I have experience with), plus I have a strong history of navigating medical systems ranging from the various jargons/codes to expectations typical in a variety of situations. These have given me some sense of how to gauge changes in my suffering over time — what may alleviate or aggravate, cycles, paying attention to trends over 24 hours, etc.
It’s not yet clear how prominently c-diff will feature in my life…it could resolve without further incident, it could happen again, it could be that I never return to the normal I knew before this diagnosis (or so I’ve been told). So I added this to my purse reference:
Line drawing approximation of how I relate to medical events impact on my overall health and likely trend to death. Adapted from Being Mortal (2014) by Dr. Atul Gawande.
This is the path I’m on (I think). I try to keep it as close as I can to the people I love, and I know that I am on my own journey which will have an end. I’m taking high potency probiotics to rebuild my digestive biome, I’m drinking viscous orange psyllium fiber supplement, I’ve changed my diet to be gentler on my system (no dairy, no fats, no raw fruits/veggies), and I’m awaiting a CT scan to check on my colon (although my liver also seems to be stressed). I’ll do all The Things that keep my path as close as I can to the people I love for as long as the time I have. It’s my answer to the question posed by Arthur Frank in Wounded Storyteller: “If I become ill again, or when I do, how will I find ways to avoid feeling that my life is diminished by illness and eventually dying?” That’s all part of our family history together, so it’s familiar and those steps are clear. In knowing that, I am less afraid of the parts that are uncertain. In any case, I am deeply grateful to be here now.
Also, “we take each day as it comes,” has become something of a mantra in our house during these times of SARS-Co-V2. Hopefully, we’re all learning together.
How I hope reflecting on the processes of my own life helps me to engage with others.
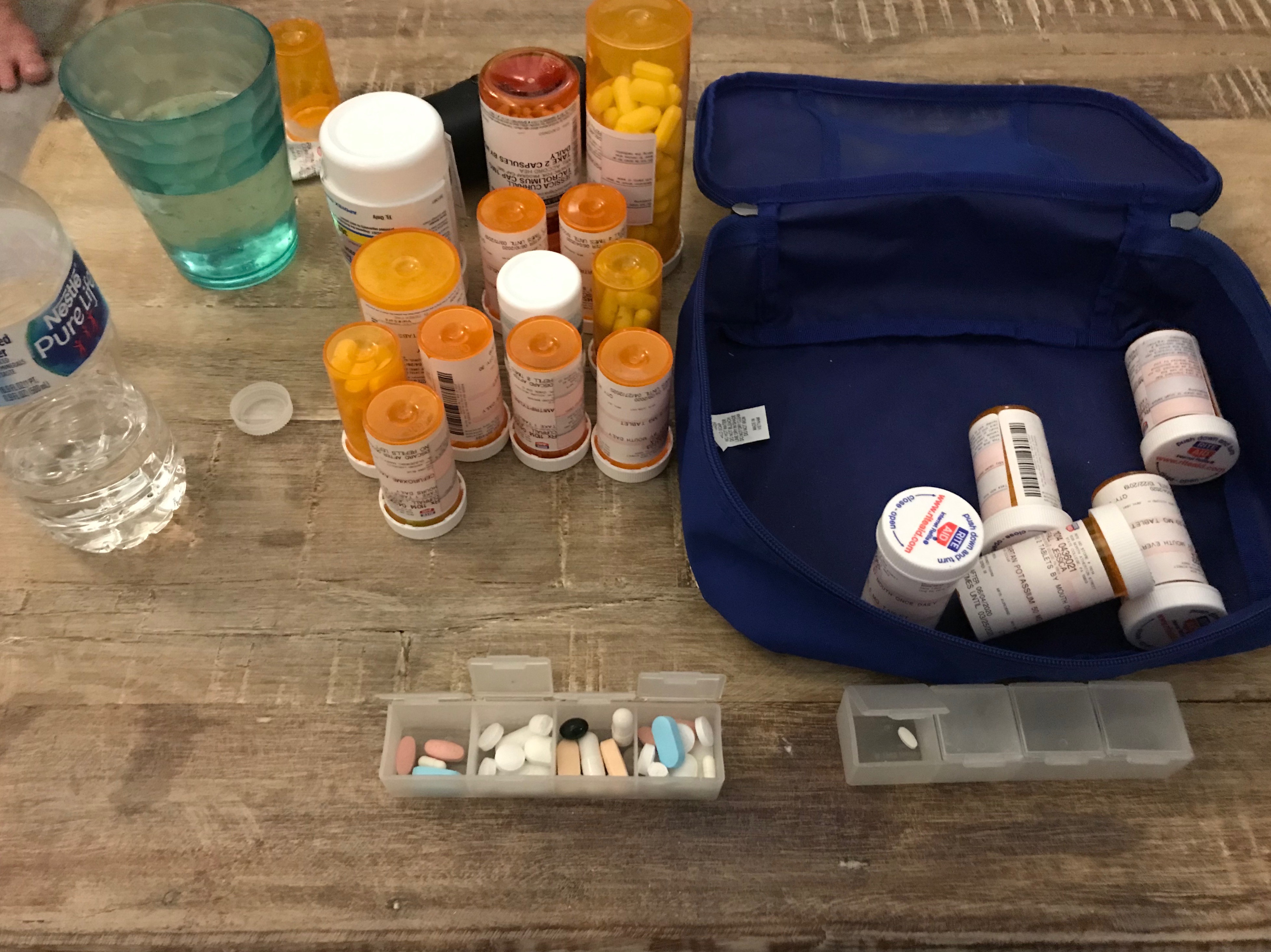
For a surprisingly long time I shared information or asked questions about my prescription management as though other people in my life also kept track of 18 different medications — not including over-the-counter (OTC) pain killers, supplements, and vitamins. It was something of a realization that I take w-a-y more pills per month (~40 x 30 = 1,200), than my spouse does collectively in a year.
When I realized that, I started trying to keep those conversations to my physicians and their teams. I bring two versions of summary tables I update with any prescription change: alphabetically by generic name which includes notes on why I am taking each, and an outline of how I take my medications across the day.
I originally tried this method because I was working with a sleep specialist and wanted to see if any of the meds I take are associated with daytime sleepiness. Then, because I already had it, I shared it with both of my nephrologists (transplant and local) and they felt like this was helpful to get a snapshot of my regimen.
Given this perspective of my day, I was described as having a “heavy pill load;” which kind of amused me insofar as I have had no fewer than 26 pills per day for over 10 years now. While this particular snapshot has more than that, at some point, what’s the difference? The gap from 26 to 40 just feels insignificant when there’s already five routine times to take meds per day. I may be able to whittle that down again, but it’s unlikely to ever return to a quantity that would be consistent with “healthy” people.
My definition of “healthy” or “normal” people are those who do not do these kinds of tasks as part of their day, or even as part of their conversations with their physician.
The thing is: there is cost and risks to not having conversations with people other than physicians and their teams.
On August 26, 2021, I went into an Outpatient Lab Facility to complete my routine bloodwork and urinalysis. As a kidney transplant recipient, that has been part of my monthly monitoring for the last decade — with the caveat that in the early days post-transplant it was every few days, and presently with the pandemic, it is sometimes more like every 6 weeks. That’s around 120 times so far and does not reflect the number of times I complete bloodwork or urine samples for other reasons; most commonly, with a suppressed immune system, I am susceptible to urinary tract and bladder infections. Are those different or two names for the same thing? It feels like I should know that, but I don’t. Also, I have a jumpy pelvic floor. With endometriosis, appendectomy, a twin pregnancy with C-section, peritoneal dialysis, and kidney transplant all in the same region surgically, I carry myself with unusual core muscle allocation. That is, I don’t always use the muscles I should and this puts stress on the muscles that are compensating that can result in spasms and cramps that feel very much like the urgency associated with a urinary tract infection (UTI).
There is no joy in learning what I really really thought was a UTI isn’t because it means:
I cannot trust my interpretation of what my body signals relay (I cannot trust myself),
I am doing it to myself: I am the reason I am in pain, and
it will be that much harder the next time I do have a UTI/bladder infection for me to recognize it.
I worked with my Occupational Therapist for pelvic floor pain relief to develop this process, which was doubly appropriate since part of the challenge was in the fine motor skills (using my hands).
The summary version of my Clean Catch Protocol is:
After I wash my hands, I tear each of three towelette packets along three of their outside edges and fold them open to try to maintain the ‘sanitary’ environment of the sealed packet.
I unfold the towelettes a little bit — only in this way are they actually usable for me.
I wipe myself down there (I’m not being coy, I actually cannot see the area I am working with), from front-to-back with each towelette separately ‘right, left, center’ and without ever letting myself ‘close’ because that would violate the whole point of cleaning. In the photo series, I used my laptop hinge to sort of illustrate this concept.
(Not pictured, even metaphorically): Pee ‘some’ into the toilet and then move a collection cup into the ‘stream’ to capture at least 30ccs.
If you’ve never peed on your own hand, it is evident that you and I live very different lives. I do not intend to be gross or crude. The thing is, part of the deal with chronic illness is accepting a level of discourse you may have never imagined for yourself. Part of coping with that, for me, is a sense of [gallows] humor. I have been greeted hundreds of times with the question, “Can you urinate for us?” If that’s not funny, it’s surreal and absurd…bordering on nightmarish.
And, as many times as I have done this, I do not understand why this is the procedure for owners of vaginas. My personal experience is that no matter how careful I am there is a HIGH probability that the sample will be considered “contaminated.” I do not know what the quantitative count of how many times that has been told to me over the years, but the emotional toll is HIGH. Is there a comparable experience quite like being told, regularly, that your every effort to be ‘clean’ with your private parts was still too dirty? The advertisers of feminine hygiene products bank on that shame.
I would also extend that this is extremely difficult to talk about. It IS gross/general or crude/rough, in part, because no one talks about it. What do persons who have more challenged motor control than I do, do with this at all? Add it all up, most importantly: How does this ever get improved upon?
I don’t just mean make it so that it isn’t awkward or embarrassing — although I would argue those are valid goals on their own — a “contaminated” result is all that it tells. There is no other additional information learned. Some of those not-a-UTIs could not be verified based on the follow-up sample; that does not mean it wasn’t a UTI. The next step in the decision-making hierarchy in that event is if I have symptoms. My aforementioned history with this pattern is a conflict of interest and credibility. Also, if this information is important, it is important to increase its success rate in providing usable results. I cannot do that on my own.
This isn’t a journal entry about my awesome specialized experience in medication management or completing Clean Catch Urine Specimens. It’s a journal entry about sharing the awkward, crude, gross, surreal, absurd, and even nightmarish with the goal that it even they can be improved upon.
What becomes normalized THEN is: Someone else will hopefully not have as complicated a time. Plus, eventually, someone else will figure out how to make things even better.
“One day you will tell your story of how you’ve overcome what you are going through now, and it will be part of someone else’s survival guide.”
Before my dad was officially diagnosed with ALS, the working theory for his abrupt weight loss was digestive: in short, he wasn’t eating enough calories. This explanation was elevated in the assessment process because one of the words he used to describe how he felt was “nauseous.” It wasn’t until I was with him over several meal attempts that I realized we needed to examine that word more closely.
To me, nauseous meant an unsettled feeling in the stomach and a pronounced urgency to throw up; I associated it with a franticness of wanting to find some where to vomit, not on myself. But my dad wasn’t doing that — he would say he was nauseous and then lie down. I believed him that his body was giving him cues and that he was acting on those with personal expertise, and I wondered if there might be other words that better matched his experience. While he rested, I did a search on synonyms.
Screenshot of a Google search for “nausea synonyms” identified: sickness, biliousness, queasiness, vomiting, retching, gagging, travel-sickness, seasickness, carsickness, airsickness, motion sickness. These were said to be “From Oxford Languages”
The two that jumped out at me were biliousness and queasiness; ironically, since these were both in a paler font. Others were associated with specific circumstances (various kinds of travel or motion sickness), which also gave us the idea of making comparisons between how he felt at that time in references to past situations of being unwell.
When we changed the conversation to add specificity to his wording and detailed comparison and lack of similarity from other circumstances, it started to change the direction of our thinking. Unfortunately, it took a little longer for his familiar medical team. They weren’t ready to rule out digestive concerns, and it took my dad’s sense of himself + his understanding of his rate of change to compel a different team into re-examining the available evidence. I also believe that another factor was the urgency expressed by my cousin to the ER doctor in the hall, making it profanely clear that her background as a nurse and knowing my dad was a clanging alarm bell that she intended to have heard.
I believe that the words we use matter. What I don’t know is whichwords most accurately convey information which can be translated when it is needed most. Sometimes words chosen can light the path to a solution, and sometimes it is a misdirect that increases pain and suffering.
Regina Fink, RN, PhD, AOCN has studied pain assessment, and has compiled the WILDA approach:
Words to describe pain
Intensity (0 to 10)
Location
Duration
Aggravating and Alleviating
Dr. Fink provides a detailed and helpful analysis of each component of the in the 2000 Baylor University Medical Center Proceedings titled, Pain assessment: the cornerstone to optimal pain management. It is well worth reading and I highly recommend it. I have strong opinions about the use of intensity ranges as the sole quantifier of pain/concern which I have gone into detail about elsewhere. For my purpose presently, I am focusing on the first section she discussed relative to words to describe pain — she goes on to explain how these lend insight in ways that are associated with nerves, muscles, and organs:
Word bank of terms to describe physical pain which includes descriptions of neuropathic discomfort, somatic, and visceral. Each category have different ways they locate and behave in the body — such as specific to one spot or across a general area.
In terms of health literacy, I feel like these are the seeds of a glossary we should be talking about, at a minimum, when relaying our experiences of pain to medical teams. These also are critical to be teaching our kids relationships with their sensations so that they are able to interact with confidence and autonomy. A shared vocabulary is critical for a culture of informed consent.
In talking with a dear friend about the WILDA approach, she asked two incredibly important questions:
What about non-physical pain? The WILDA vocabulary do not apply well to mental, emotional, social or spiritual/existential pain. We agree that it is misguided to conceptualize these as exclusive or can be distinguished from one another.
How do we move beyond a comparison of pain against NO-pain? If zero discomfort is the standard of ‘normal,’ both she and I are immediately out of the conversation because that does not happen for either of us.
I don’t have an answer to these questions even just for myself, but I do know that I benefit from conversations about it and that sometimes having a starting place to bounce off of helps advance the cause.
A book that has been helpful as a parent is Maria Lamia, PhD’s Understanding MYSELF: A kid’s guide to intense emotions and strong feelings (2011).
Dr. Lamia’s review gives broad descriptions of emotional landscapes and provides key words that may be associated with these. Each chapter includes information in straightforward language, first-person kid quotes, a short survey of self-evaluation, resources for building resilience, and some research-based science. There’s part of me that experiences my pained and suffering Self aschildlike…that I do best in understanding, relating and creating spaces for healing when I can hold myself gently in that mindset.
I reviewed Dr. Lamia’s vocabulary for the areas of Feeling Self-Conscious (which includes embarrassment, guilt, shame, and pride), Feeling Threatened (as with anxiety, fear, and disgust), and Feeling Gloomy (loneliness, sadness, and grief).
Note: I kept the terms for Pride in the table, but I tend to associate that as a positive and I am not sure how that would correspond to medical/mental health teams at least in the same way as the other feelings and emotions.
A table of vocabulary grouped by Mary C. Lamia (2011) categories in columns of Feeling Self-Conscious, Feeling Threatened, and Feeling Gloomy. The second row includes additional words from my own experience with feelings, social implications, and thought energy flows I associate with each column.
With my kids, I can just turn to the main chapter grouping and have them review the words — typically, they find that there are a few that ‘jump out at them’ almost as if they were written in a special font at that moment. Now that they are teens, we can talk more about the nature of their thinking — are thoughts like ping-pong balls, bouncing out of control? How about circling around or spiraling outward from a central, negative idea? Maybe just stuck and unmoving?
I say this is something I do with my kids, which it is, but it is as much a process I am trying to learn myself as it is something I hope to impart as a parent.
Two photos of the same tree. On the left, it appears round and full. On the right, it is evident that the trunk and crown are actually U-shaped with an enormous gap in the leaves for where it has been pruned back for power lines.
So that’s where I am with this, fully aware that this is not a whole picture.
I do not yet have vocabulary for really any social or spiritual/existential pain — although I suspect there is some overlap within aching loss and/or feelings of being outside of a higher order of belonging.
I also know that there are cultural differences in the experience of word meaning particularly as it relates to co-constructed understanding as with exchanges of information. As one example, being white may have had an influence on my cousin’s use of profanity as being heard as emphatic and passionate rather than with implicit biases of being unsophisticated, threatening, or disrespectful. Conversations among speakers of the same primary language undoubtedly go more smoothly than when there is a translation involved — particularly when some languages may not share common meaning in expression or tone. The very real risk is informed consent may not be achieved, and in medical-health situations that rapidly becomes dangerous.
I want to do better: I want to learn more. I want this to be just a beginning.
My earliest memories of being “not-well/whole” were both in 1982, when I was 8 years old. We were traveling in Mexico and at that time, water was problematic for persons not from the area. I remember clearly seeing the red tomato soup and orange soda before vomiting all over the restaurant table. I don’t have a visual memory of what happened next; only the sound of one of my parents chiding me for not going into the bathroom to throw-up, and the other parent chiding them that I probably would have if I’d known what was coming. Lesson: Whenever possible, be discreet with sick: others don’t want to see that. This was confirmed many times over the years by peers, educators, and faculty at every in-school vomit I ever witnessed.
Later that year, I took an abrupt fall on roller skates and ‘caught’ myself poorly with my left hand. There was a bracelet of bruise and I couldn’t move my hand, but it wasn’t swollen or at unusual angles. My parents and I went to the nearest Emergency Room, and I knew that they weren’t happy about the option because it did not have a reputation for quality of care. It was just the nearest one. Lesson: a person in pain may resort to the available response, not necessarily one they like or want.
I don’t remember anyone talking to me. I was wheeled into the x-ray room without my parents, and the technician kept positioning my broken wrist in ways that made me cry out. In retrospect, as an adult, I know he was doing that to get images of the breakage, but I think the only thing he said was, “stop screaming.” Lesson: Whenever possible, be discreet with pain: others shouldn’t have to deal with that. This was confirmed many times over the years by peers and family as soon as I joined the club of menstruators.
Thinking about it now, I didn’t have a pediatric dentist — I have no reason to believe that was a thing when I was a child. I saw one of parent’s dentists, who I have no recollection of ever saying anything to me other than to tell me I needed to brush more and floss. Lesson: Experts knowwhen you aren’t following the rules of care, and will call you out if you lie.
I have vague memories of appointments with some kind of vision specialist for awhile. I have no idea, none whatsoever, what the goals were — watching rapidly presented photos of dominoes and told to call out the numbers, use a mirror to draw myself…I remember crying a lot. The man got upset with me for getting upset, but if there was a lesson in there somewhere I missed it entirely.
In grad school I saw someone for chronic migraines — my primary care physician, a headache specialist (is that a thing? I developed elaborate rating scales to note + characterize my daily pains and what, if any, patterns might be detected for catching when a headache was going to turn into a migraine so that medications that worked best in the first hour would be effective at all. Lesson: More data doesn’t necessarily lead to better answers and sometimes the answer medications offer isn’t much of one.
After grad school, I worked as a speech-language pathologist in a school district. Being a part of hundreds of meetings and forests of paperwork, I was the “expert” that was supposed to explain things — clear communication was my job. With all those kids, parents, educators, and other special area people, I developed and refined a sense of how to filter information, translate jargon, take notes, and ask probing questions. That inadvertently served me well when I became catastrophically ill. I’ve already written about my medical diary and questions, so my main point now is that I came into a process of learning how to navigate my body and interactions with others when unwell became explicit, intentional, and collaborative.
I wasn’t just showing up with my body of evidence for someone else to tell me what had happened, was happening, might happen next. My being chronically ill pretty well exactly paired with my parenting, and over time I began thinking more and more about explicitly, on-purpose teaching my kids along with their other parent and medical teams they encountered.
we talked about them over dinners, read excerpts together, referenced these ideas when current events featured health or medicine, and practiced increasing self-advocacy with respect to their own medical-emotional health.
Sometimes it was an overlap between my health and this goal. As in, it was during the time when a new blood pressure medication was making my vision blurry that I realized I shouldn’t be the one reading over the counter medication labels for them: as teens, it was appropriate that we should transition to supporting their decision-making in listening to their body and taking steps, knowing about dosages and timing schedules.
The only thing I might add to Figure 4, Model 13 from my personal experience is
a loop — that this is a repeating cycle, not finished in the way “conclusion” often implies, and
some vehicle for storytelling: sharing lessons learned with others, hearing and learning with theirs.
For me, the sharing component is similar to “Balancing between hope and despair”: it is a filter or prism that influences all of the other aspects of preparative waiting. The figure in the hall, the patient, in so many respects may be alone. However, there are resources to be found within their framework of preparative waiting:
to have heard about the seeking and giving of information in medical-emotional health experiences of others (e.g., this is what happened with me),
to know what kinds of clues there might be and perspectives of interpreting (that is, how I saw, heard, felt, came to understandings, etc., along the way),
community references around cultures, spiritual and philosophical practices in handling the existential threat within “why is this happening to me” and “what does it mean?”
and giving and receiving among one another meaningful support and tools for establishing spaces of calm within the inherent chaos and uncertainty whether or not respite is sought. Rest from thinking, wondering, imagining, dreading, worrying, grieving; recuperation from all the moving around that comes with being acted upon (even in the service of diagnosis).
Towards that end, I find myself at this end: it is time I rest my mind from this.
At the time of my first experience with catastrophic health failure, there was a popular t.v. show which featured a gifted but cantankerous diagnostician who got all the most problematic medical crises AND completely solved them within the hour-long drama. The show’s focus was on the physician and his process, and it was seductive to celebrate a genius-healer (comically gruff none-the-less). I imagined that if I were truly sick, I would accept the expertise of anyone to be well, no matter how rude (cruel) they were to get to that happy end.
When I became the problematic medical crisis, part of the unraveling was the absence of heroes and heroics. As the many hours became many years, I came to an altogether different understanding about what I wanted of a physician and medical team, what my role was, the drama trauma tedium of the process, and if it ever ends. It’s pretty clearly that would not be an entertaining show.
The back of my right hand has a visible path of bluish veins, and, following those lines, a constellation of small whitish scars from where intravenous (I-V) lines have been established.
Medically speaking, if there is some choice to be made, choose to be boring. Being interesting or a ‘learning experience’ for someone else isn’t awful, but it’s not ideal; and being a challenge to a medical team is downright crummy. I am not of the opinion that I can separate my sense of my self (my identity, my value, my presence) from my body (which necessarily means my illnesses). My body is the vessel by which all of the rest of it exists in the world. It’s one thing to explain this to other people, it’s a whole different conversation with medical teams — often specialized to really only recognize a part of me. I don’t want to be difficult.
On Twitter, I saw a compelling contrast of statements. Unfortunately (1) I cannot find the original post that I saw this, but (2) it is common enough that it should also be familiar to medical teams:
From the physician: “Your online search does not compare to my medical degree + years of practice.”
From the patient: “Your medical degree and years of being you does not compare to my years of living as this Body Self + particular concern which drove me to research it
I have a strong professional background in data collection: I have spent significant time studying not just how to do it but also how to teach it to others in clinical practice as a speech-language pathologist. In short, I know the value of being able to look at a set of information and interpret it easily. However, when applied to myself, I was told I was a “type-A personality, which is more likely to experience anxiety, perfectionism and control issues.” If I enter a conversation about how/why I charted things the way I did, I run the risk of validating that off-the-cuff assessment and overstaying my allotted time in the physician’s schedule. So I made a different choice: I don’t want to be difficult.
Aside from when I am characterized with a personality profile directly during a medical interview, am I noted as responsible, thorough, informed, educated — a self-advocate and collaborator of my own health? Is there a working theory that I am medication- or solution-seeking for situations which have none; that is, when there is no cure which completely solves the problem in a tidy way? It all runs through my head (and more) when I am trying to navigate from the inside of my body self.
It is as familiar as the back of my hand.
I find having intravenous (I-V) needles in the top of my hand intensely uncomfortable. There isn’t much flesh there and when I am dehydrated, which commonly happens before any procedure with a no eat or drink restriction prep, it is harder and more painful. When push comes to shove, it doesn’t much matter though: because I don’t want to be difficult.
End blip.
Note: among the biases I face according to my age, gender, and particular health profile, I am simultaneously aware that there are different and huge forces that threaten “difficult” over other persons on the basis of their age, gender, race, faith and cultural background, and health statuses. I do not know what the answer is, but I am ready to listen+learn so that I can do my part in making this better.
I do not remember childhood feelings of shame or unworthiness in a global sense. Within specific circumstances, sure: but as a kid I felt loved and I believed it. Sometime in middle and high school things became less hinged between my parents and I, but not in a desperate or flailing or failing way.
So let’s say the beginning turn was the intersection at becoming a parent Chronic Patient.
I wish the signs were as easy to see.
There were other things that happened simultaneously — that was when some of us recognized my mom’s problem solving and memory skills were inarguably abnormal. Plus I had to adjust my expectations for myself relative to my job; coming off of maternity leave and being a working mom with a stay-at-home working partner as primary parent to our twins. While clearly these have significance, they happened outside of my body. Newly being a parent + Chronic Patient both came from within.
What I remember about the first night of congestive heart failure was more nagging worry. The cough wasn’t going away, and I couldn’t quite settle. I didn’t know then what I know now, so I wasn’t afraidof it, I just didn’t understand.And then I didn’t understand all the fuss at the emergency room, or how the babies would be fed once nursing was not available to me (or what to do about all the milk that just kept coming), or when I could get back to my family, or what the terminology meant (not ‘failure’ like your heart failed, but it failed to keep up with the level of fluid overload…), or how sick was I: is it really safe for me to go home? What does it mean that I am the youngest person by twenty years in the cardiologist waiting room? And so on.
I do not recall dwelling on the questions, just that I had them and they also dissipated. There was always so much to be done, it’s not like there was a ton of time to think. Routines got carved out, we moved on.
What I do remember about not dying in 2009includes asides from the particular question of when/how/why shame developed.I remember feeling there was no dignity in catastrophic illness, and no need for it. I had no control over any bodily fluids, vomiting or diarrhea were irrevocable. Going to the bathroom lying down while on dialysis was the only option, so that’s what I did…apologizing and thanking the nurse who stayed with me and cleaned meafterwards.
There were a handful of magical thinking episodes, and among them was the dual notion that: I got to be alive to see that my spouse and kids would be okaywithoutme, and that my part going forward was to not to make it harder forthem. Those are the words of the mantra I told myself but I think the underlying meaning was:
I have no value to my spouse or kids, and
I am already a problem/difficulty, but TRY not to make it worse.
Except, I was always making it worse.
I was desperately afraid of bankrupting our family with my medical bills. That we would have no college funds for the kids, no retirement fund, we might lose our house. In my mind, the cost of my being alive was astronomical. I told myself, repeatedly, I would never live long enough to be worth what had been given on my behalf.
This was a water color painting I did of my backyard. It started out so different from this, a collage with strips of construction paper (while still being my backyard), that when I saw it come forward like this I actually gasped.
So maybe I am more sure when/where the shame started…but knowing it was me all along doesn’t quite feel like helping. My back yard, metaphorically and actually, isn’t moving.
I realize that I have memories of more Body-Self health stories along the way. Some scenarios that grew from thoughts that I presented to myself and did not question. Others were explicitly directed to me — chided for taking on too much fluid before dialysis, for example, was received as a brutal judgment against thirst. In addition, another setting evolved within my job and although it was outside of myself, I internalized the work I did there.
The first three years, I’m pretty sure I loved it. It was hard, but I thought I was good at it — and particularly skilled at some aspects of it. At the threshold of 2012, another unanticipated intersection: I wounded a critical place on my arm in a random, hapless accident and the funding for my position at work changed, shifts that gave me wholly different perspectives of myself.
I had been excited to go to that performance review — a chance for someone else to see what I had been dedicating myself to doing well. My wrist was unnaturally bulged and throbbing, so I kept it on my lap out of sight, under the table. The meeting began with an immediate pivot into the bureaucracies of University existence. I’d had no idea, did not know what he was talking about. “You’re completely outside of all metrics.” “All of this is essentially invisible as far as the University is concerned.” Are you telling me that I have not been describing what I do in ways the University recognizes, or are you saying what I have been doing is not my job? “I’m not sure.”
I didn’t ask this out loud, but my mind rattled with: How could I possibly have been working so hard and yet it was abjectly irrelevant? I have a feeling his response would have been, “I’m not sure.” In my mental timeline, the surgery to end my fistula was near around then, and the two incidents are pretty well merged in my mind.
Content warning: the next photo contains a wound.
Unbeknownst to me until I woke up after, the surgeon used glue instead of stitches in the procedure to ‘tie off’ my fistula and resolve the aneurysm that had developed when I bumped a doorknob. To me, the result looked as though I’d been attacked by a hatchet.
A lot of things happened between 2012 and 2017, which is when I decided I wasn’t a good fit for the position (I really wasn’t), and it wasn’t a healthy fit for me. There were so many conversations where, in so many ways, I did not know what was happening. Brain fog seemed to be constant. Dreams were consistently horrific. Incontinence, pelvic pain, and sudden loss of bowel control all sure seemed like they were related but endless appointments with specialists and increasingly bizarre tests never identified a thing. Work aspects I thought I did well were evaluated otherwise in blunt, unambiguous and minimizing terms. My mom died in February and by March I said that I did not think I should return to the position in the Fall.
I never quit the position: I was never offered a new contract for the next year. The bureaucracies re-surfaced and I wrote a letter. In all that time, not a single licensed person ever observed me and gave me feedback on my performance on half of what I’d understood my job title to be. I had no ‘exit interview’ — no one asked what I learned, or what I might’ve done differently. I infer that none of that was important enough to matter. I remember so much confusion and weeping.
I’d wanted so badly to be a recognizable wife and mother — to be trustworthy. I wanted my doctors to consider me a “good patient” and not just care for me but also care about me. I strove to be a contributing employee. I wanted my mentees to know I took the situation in deeply. I liked feeling that my experiences had purpose — that my first-person knowledge gave me insight, meaningful perspective. That my struggles and my victories were visible also to others, and mattered. But maybe neither were.
2021 marked the four-year anniversary of when my mom died, abruptly of an intracranial hemorrhage (February 2017). I had learned about dementia before then through a support group for adult children of aging parents, so our last year or two of interactions were much improved (even if often odd). My dad died of ALS something like two years and one month later (March 2019). All of that and the year afterwards was intense and surreal. Many times over we said out loud how glad we were I had not been working.
Now I am spending hours most weeks thinking about sleep/dreams, and trauma. Trying to unravel who it is I am today, and what all that means particularly as it relates to who I would like to be — separate from any “shoulds”. It feels like some of it is finding a path to resolution, but I’ve been pretty convinced that walk needed to include a reckoning with myself: hence this entry.
Winter of 2021, a group of three deer wandered through our back yard.
It’s still me. All along. I see that there’s more than shame back there, but I don’t know what, if anything, it all means. For now, I think that’s okay. I’m going to pause on these thoughts, and explore others.
For awhile now, I have been working to refine my sense of physical and emotional suffering, which I termed globally as pain/concern. More recently I have been trying to wrap my thinking around a different combination of physical and mental complications. My assessment of whether or not I can do something, am successfully doing it or need to adjust immediately, or believe I cannot do it and will not even try includes: anticipating pain or task failure, in-the-moment pain or mistakes, and backlash either as regret, ache, or a mess that shows up later. It’s a heady mix of questioning strength and confidence.
On the first warm day of 2014, I tried to put up the porch table umbrella so that we could eat lunch outside. It slipped & the angle shattered the table into a gazillion shards of glass which completely covered the porch + fell into the rocks/grass below.
What I remember most clearly about the moments immediately after when I had destroyed our table, was that it had not in any way occurred to me that I couldn’t do this on my own. I had retrieved the umbrella from the shed, carried it across the yard + up the porch steps, held it over the height of the table to position it in the center…
I had done this before — it was not a new task to me although it was typically only once in Spring install and one-time removal in Fall. I don’t think I knew the table was glass. It never occurred to me that it could completely crumble into a gazillion sharp edged pieces…
Also, I was in somewhat of a hurry. Food was in some stage of being prepared, the 8-year-old twins were ready to eat. I couldn’t let them anywhere near this. I didn’t want anyone else to have to clean up this catastrophe. I kept imagining bloody footprints from yard creatures getting cut by my gross err in judgment.
Worse still, I was not physically capable of cleaning it all up. I became dehydrated and light-headed, the glass was too heavy, the sunshine blazing. I was so deeply sad that I had to give it over to my husband. It all felt awful.
In August of 2019, I was picking my teens up from a summer art camp, and completely missed a step at the front door of the building. That fall lead to a broken wrist, with a radial plating system surgically implanted.
In the moment, I did not see the fall at all. I know I witnessed it at a subconscious level because it was returned to me in dreams later. Had I noticed the step, I am sure I could have been both physically strong and entirely confident = successfully completed the act without injury. But that really does not matter because that’s not at all what happened.
Sitting on my couch right now, I cringe and fix my jaw at the memory of it even still. My sense that I will see the potential problems feels pretty unreliable. Where do strength and confidence go?
If these kinds of categories were to get added to the Tell Me About Your Pain/Concern, how would I quantify anticipatory pain/worry? I have used the terms “ominous” and “dread” to physicians and physical therapists; as in, “I have an ominous sense that I am going to have severe heart burn from my potassium supplements, and I have to remind myself to relax or it is more likely to get stuck in the tension of my throat.” Or, “I know I am carrying myself very cautiously on walks because of dread that I may stumble.” I know that this is primarily a mental-emotional issue, and it matters because it directly influences how I act in the world even for the most basic activities of day-to-day living.
Reviews of ability to complete Activities of Daily Living (ADLs) that I have often seen relied on simple scoring: 2 = could do independently, 1 = could do with assistance, 0 = could not do. While this is easy to compute an overall tally, it may not adequately capture skill sets and the mental-emotional processes associated.
In 2019 when my Dad was in rapid progressive decline with ALS, I noticed trends which were both physical and mental-emotional in him (it’s easier to see such matters in other people than I tend to in myself). There was almost nothing he could do with complete autonomy and no modifications; but sometimes it was my sense that he answered according to what he wished were the case or based on how he had done the last time he’d tried even if that was awhile ago. Together we came up with a more representative set of characterizations:
5 = ABLE TO DO without apprehension or concern (e.g., not afraid of pain, falling, etc.): If he was already seated or lying down, he could use his telephone for brief calls.
4 = Able to do WITH CAUTION and CARE (that is, some discomfort likely such as strain or queasiness, may require pacing or preparation to complete). He could complete oral care tasks from a bathroom seat. He could consume protein drinks by straw. He had prepared his tax filing documents just before he started struggling more prominently, so in that sense he was well positioned with his finances.
3 = Able to do ONLY with strategizing ahead of time to break task into level 4 component steps; “warning” discomfort expected; must manage remaining strength and energy. In terms of managing medications with respect to dosages and times, this was probably at a 5; however, actually taking pills required numerous steps by others (assembling, crushing to powder, mixing in with applesauce or pudding), and also himself (remembering safe swallow techniques, pacing energy consumption for sitting up, etc.)
2 = ONLY able to do acknowledging IT WILL BE UNCOMFORTABLE + depleting. Pain + queasiness present at distracting but manageable levels. Energy depleting. Weakness is distracting. Walking with a physical therapist was dreaded even when at an emotional level he valued the concept; transferring into and out of the wheelchair.
1 = MINIMALLY able to do; SIGNIFICANT CONCERN: Toileting was a tremendous issue.
0 = UNABLE to do; UNIMAGINABLE: the idea of walking down more than 3 steps, doing laundry, and driving were all extremely complicated physically and cognitively, all bore very high probability for serious injury to the point it really wasn’t worth debating.
There are a number of standard ADL lists that I did not include in this because they weren’t relevant to my Dad’s life at that time — cooking and housework were not part of his daily life.
As I reflect on all of this now, I can see how these rankings incorporate both
the physical demands of the task, which includes capacity, strength, stamina, persistence and
a sensibility of prognosis: based on (recent) past experiences, what confidence do I have that I can do this successfully.
Said differently, how a person gauges across both of these that they can start, do, and complete something without needing someone else, and without having an accident which makes a bigger problem as either a mess or an added injury.
For as much as I dislike the anxiety + self-doubt of anticipating pain or task failure ahead of an event, the other end of this gamut is achy backlash, regret hangover, or aftershock. It is nerve pain that feels EXACTLY like a bee sting when I am brushing my teeth at the end of the night, knowing with certainty that I have not been stung but rather this is a residual complaint from an aggravation I did not notice at all in the moment it occurred. It is waking up the next day unable to turn to the left after carrying heavy groceries upstairs (maybe that’s what it was?). It is overwhelming guilt that maybe I will not go sledding with my kids next time because this time many muscles and joints hurt so, so badly by dinnertime. This may be the most debilitating of pain/concern because it lands so deeply in my ocean of shame. It is in these moments where my sense of myself — my personal metric of strength and confidence — is most challenged. Activities that do not come with a delayed pain/concern do not register in my memory. As a result, they contribute a much quieter impression of what I can do successfully.
As I read over all of this, I am reminded that my attitude about developing a Tell Me About Your Pain/Concern scale has always been as a tool for communication, patient advocacy, and health literacy. I’m not developing a screening measure or billing code where scaled numbers are calculated vertically to a singular number. What I really hope for all of this is to promote a broad-based framework towards productive conversations and those get individualized (more narrow) with the follow-up questions. With this in mind, characterizations about fear and quality of life could be immediately linked with further investigation of the role of strength and confidence.
It also validates making an explicit practice of “I did that” recognition — making sure that these become part of my history of me. This could be paired with explicit practice in low-stakes tasks: identifying when I have moments of doubt, and exploring those experiences in ways that I can readily find the boundaries of my strength and confidence. I may always have <5 ratings within my activities of daily living capabilities — may those be opportunities to build, broaden, adapt, and share with my medical/health care team.
The first time I was hospitalized for congestive heart failure, I was almost given twice the medication I was supposed to have at 3am. As soon as that was resolved, I grabbed the notebook that was beside the bed and started writing everything down. That was the beginning. Since that time, not quite every single place I go, I bring with me a notebook. In it, I have all of the phone numbers of my physicians, a copy of my medical history in outline and my current medications (usually 2 copies, so they can just keep one), and a list of time-tested questions in case I freeze up and forget to ask.
It helps me to remember that Brain Blank is entirely neurological at the most primal levels — it’s not that I’m not paying attention, or that I’m not smart enough, or even that my doctors are necessarily callous/over-hurried but that the brain copes with shock in incredibly unproductive ways (even small scale shock like being asked a question unexpectedly as in pop quizzes). There is a flood of cortisol and adrenaline so that you are ready to fight/flight without thinking, and that, by definition, turns off any part of your brain that would come up with good questions. It will also greatly minimize the likelihood of remembering the answers, so it truly truly is natural and normal to feel like medical appointments are a blur. Add to that sustained ‘shock’ like pain (either chronic or acute), stress of Life stuff, and the combination is pretty brutal in an exam room with the paper sheet and the dysfunctional medical gown. In sum: Having the notebook gives me something to do, which provides emotional distance, but mostly it means that I have something to refer back to when I come back from Paleo-Mind.
Before big appointments, I write out all of my questions and review them with my spouse (he often thinks of things I didn’t). I also rehearse and model this with my teens before their interactions with medical care teams.
For a telehealth visit on 21 January 2021, ahead of time I noted my vitals (a.m. & p.m. blood pressures from prior day, temperature & weight), and the questions I wanted to cover in our conversation. I emailed all of this to the physician ahead of time for their reference along with my most current prescriptions + schedule of when I take them.
The thing is, sometimes it is a challenge to even know what I should be asking about. I do not know the names for all of the parts of me. There are situations where I cannot see or ‘point to’ where the pain/concern is. I try to use a guide of presence (that is, “what are the circumstances when IT happens”) or absence (as in, “what are the circumstances where I WANT it to happen and it DOES NOT”). Even that can get twisted in a hurry: I have no basis of comparison from if other people experience the presence or absence of something the way that I do to know if what I am saying will contribute to meaningful problem-solving. The nature of my illness has included conversations I never imagined having (e.g., how often and how much I urinate), to conversations I desperately need to have but are taboo (such as how fatigue impacts libido in a partnership with someone who does not have chronic illness).
Anatomical photo of female digestive system + pelvic region with organs, muscles, and nerves labeled. Post-it notes with observations & questions are on top of areas of concern.
I try to come prepared to learn about my body and the care/keeping of it. I bring in materials to support conversation so that I know there is shared understanding of regions of the body and what to call them. I have asked “how can I be a better patient?” with the intention of advancing my understanding for future visits, or alerting the physician that I feel we are in an ineffective dynamic. I used to feel like a failure and a freak if the visit ended without resolution. If the specialist had no idea what I was talking about, it must be my fault. I absolutely do not believe that any more; however, that’s a journal for another day.
Before I leave almost all appointments I say the following: “Let me read back to you what I’ve written down and make sure I’ve got it right.” Because that’s my ritual, doctors who I see regularly know and anticipate this; and it’s a habit I’ve practiced so much, I really have not walked out of a room without at least those answers. I still get sprung with unexpected information or questions, which I hate like a pop quiz; but I have a specific plan and that has gotten me through. If during that review a doctor interrupts/corrects me, I write that down, and go through the whole thing again. My cynical side also feels like this has established me as a much more serious self-advocate than I might otherwise be, and since I am navigating across many, many specialists there have been a LOT of times where I could provide information (recommendations, dates, etc.), faster than they could look up in my file. It also means I have clear info to compare with second opinions.
The back page of the notebook I keep in my purse has questions that are consistently useful to me even if I cannot think of ‘new’ questions in the moment. Even if all I remember to do is ask these + note the responses, I feel better prepared.
My “generic” questions are: GENERAL (1). What should I do to take care of myself? (2). What should I expect over the next few days? (3). Is there anything I should look out for (red flags)?
MEDICATIONS: (1). Tell me about the side effects: headaches, sleep, mood, sexual, weight gain/appetite/nausea, dry mouth? (2). Interactions with other medications (3). When might I anticipate change?
The answers to my General and Medications questions help re-orient me to being active in deciding IF I am going to pursue recommended next steps OR the conversation needs to continue (sometimes with another physician entirely). It is in my experience existentially critical to remember that “No, I’m not going to do that.” is mine to inhabit; it is true, and important. Knowing what my health status is and what my standards for quality of life are is critical to surviving and, ultimately, living -– those are not the same thing. Over the years I’ve come to rely on what I call the 4+1 questions as a structured way to think through recognizing and declaring when I am at this point.
I’m feeling tired, so that’s all I’m going to put for now.