Very often this online journal has been a place for me to explore my thoughts and experiences. I keep it ‘public’ because I believe that sharing our stories with one another allows us to learn better and more collectively.
Recently I realized I had quite a few photographs that may serve to illustrate ways to interact with elders.
There had been a steady decline. The first time we met, he was sitting in a chair with a walker nearby. Then the chair was a wheelchair. Next, sitting up in bed. Now, he lies back even with his eyes closed.
He said, “I wonder where the deer have gone.”
“Deer?”
“Yes.” He explained, “I used to see deer from my window here.”
As of this moment, I do not know if that was our last conversation. Maybe we will talk more this week about one thing or another. I have quiet in the not-knowing, and that is enough.
nurture memories of your mother’s rose garden at the side of the house (when you out grew the swing set), of standing barefoot in the dirt eating warm and dusty cherry tomatoes, of visiting botanical gardens, of discovering sculpture gardens, of walks in the neighborhoods to admire what others are growing (the neighbor who recreates a meadow filled with more flowers than I can count, the one who artfully fills every space with vegetables in raised beds, the one who welcomes pollinators),
share page-turning in catalogs for seeds or landscaping and say “ooh…” or “wow!” at the different colors or styles or seasonal arrangements,
hear people who know “Jean” well mention that, before the ALS, her strong knowledge and skills in plant care would’ve found her in the yard most of these sunny days of late,
read Todd May passage about practice in ancient China of friends from childhood writing to one another over the long years as working adults (when they lived apart) to collaboratively imagine the garden they would one day come together to create and take care of in retirement.
Instructions
Prepare mental model of conversation method: 3 options spoken as a list, then repeat with pauses after each one to monitor for response. Note: Watch her eye gaze for indications that short-term memory has faded and a repetition may be warranted.
Practice consistently with simple tasks: “Do you want to keep watching t.v., listen to music, or something else? Watch t.v. [pause], listen to music [pause], something else [pause].” It becomes a structure I can think in and she knows to anticipate about me.
Talk about the birds at the bird-feeder together. It’s present, so can be referenced directly. Be open about when I did not understand. Laugh together when we are both startled by them abruptly flying off and then their gradual return as they realize it was just a noise. Joke about how flighty birds can be.
Describe the flowers in my yard that I do not remember the name of. Listen and watch carefully. Brown-eyed Susans. Recognize that she is right.
Tell the story about friends designing a garden together and invite what kind of garden we could design together.
“Should we have many flowers everywhere, a few flowers that we can focus on, or something else? Many flowers [pause], a few [pause], something else [pause].” Many flowers.
“Water is nice. Should we add a fountain, a fish pond, or something else? A fountain [pause], a fish pond [pause], something else [pause].” A pond.
“Will there be vegetables in our garden? Tomatoes [pause], carrots [pause], something else?” Maybe.
6. Realize and say that, so far, she is doing all of the actual gardening — we’ve already established that I don’t know much about plant care. “I’m not sure I am contributing. I’m happy to be beside you and learn but I don’t know what I can do for us. Maybe I can pick out the hats we wear so we do not get sunburn.” She smiles.
7. Realize and say that in an imaginary garden, there doesn’t have to be sunburn. We laugh. “Since we can do whatever we want, what else are we going to get rid of. I vote no mosquitos.”
And no bees.
The thing is, me, on my own: I am okay with bees. I am not allergic — I don’t recall ever having been stung. I enjoy their flight and dance, I very much appreciate what they do for the flowers. But this isn’t about me.
The notion of agreement implies plurality: there is an inherent “more than just me” to the word because, on my own, my perspective of the world is my default setting for what is real. I don’t have to agree with myself, it is my baseline of relating to the world. However, in any interaction with someone else, there are points where we have very similar perspectives and also those where we diverge. This is not the same as having a different opinion (I think vanilla ice cream = awesome, and for you maybe raspberry sorbet = awesome), but as a more fundamental sense of what is occurring. In spending significant time with persons who are in hospice care, I have reflected a lot on what it means to be in a shared space across more than one experience of reality.
All of the people I meet in the course of volunteering have one or both of the following characteristics:
altered sensory perception such as pronounced hearing loss, vision impairment, motor changes that impact how easily/often they move, changed proprioceptive awareness (processing their body in space), and/or
diagnoses of dementia (often exacerbated by the challenges with sensory perception and routines of life in a facility).
These cannot be separated from one another. Each informs the other.
An incomplete list of factors which can influence each of our experience of reality.
Example: Once while visiting a Friend, I noticed she had received mail. I opened the envelope and handed it to her. She responded, “I need my focusers.” I found her reading glasses and she accurately read the letter out loud, commenting with comprehension on things her friend had written but stopped mid-sentence when it reached the edge of the card. I turned it over for her and she continued reading. My reality and hers included knowledge of reading glasses, literacy, and social conventions in written correspondence. We both spoke in complete, grammatically intact sentences. Her reality included a creative word use and did not recall that the back of the card finished the sentence. Neither of those are a problem for me because my reality has opportunities to be flexible as a benefit of being a volunteer.
Animation my son made for me which transforms an image of a pair of glasses into separate, abstract spheres.
The “Story of the Focusers” has represented a type of the interactions I regularly have. There are multiple points of agreement in a shared reality; what differences there are need not stress my version.
I have another Friend who has an insatiable drive to move, primarily to stand and walk, which is in dire contradiction to how unstable she is on her feet. I thought I had figured out a resolution by walking alongside her wheelchair, pushing it with my right hand while holding under her left hand with my left hand. She spoke in phrases that I would sometimes repeat (“your mother’s garden?”), but it didn’t seem to matter so much that there was a back-and-forth between us. When I sang, “Take me out to the ball game” she interrupted in the middle to say, “I like that.” It was a nice visit.
The next week, she’d had an extremely serious fall resulting in significant swelling and bruising on her face and hands. She was talking very quietly primarily to herself (in a way consistent with other visits), but occasionally turning her head as though she were directing what she said to someone not present to me. Even with one eye completely swollen shut, she kept reaching beyond the balance of her chair and leaning to shift around me sitting in front of her. I was amazed at her persistence and creativity. It was clear that she knew I was there insofar as I was an obstacle to her primary goal of getting up and that she was determined to solve that problem. In almost every other observable way, we held completely separate spheres of experience.
Last week, she was considerably healed from her injuries. There was a gardening magazine in front of her at the table and sometimes she turned the pages (left to right), and even directly responded to things I said. I posed, “Did your mother’s garden have flowers?” She looked at me and said, “No.” So I asked if it was vegetables, like carrots and tomatoes, and she nodded and repeated, “carrots and tomatoes”. Does that mean that there were more points of agreement in a reality we shared together? Perhaps. It honestly does not matter. I look forward to visiting with her next week, and we’ll take it from there.
When our twins were born, my mom came to stay with us to help. That’s when my spouse and I knew with certainty that something unusual was happening with her thinking — her memory, sense of the world, and problem solving were all unmistakably strange.
We couldn’t seem to get her to stop drinking my husband’s coffee, even though he prepared his entirely differently (black, no cream or sugar) and he bought them both different colored mugs with labels written on them (“Grandma” and “Daddy”). She made 3 packets of Kool-aid all at once, using a large bowl for one because we didn’t own that many pitchers. Her explanation was, “I didn’t know what flavor you wanted.” There were other, non-beverage examples, but the point is essentially: I didn’t understand her thinking, and I didn’t know how to relate to it meaningfully.
As years went by, talking with her consistently featured many repetitions of stories, some of which were definitely not true. As the twins got older, I worried they would be confused by these patterns and that the other adults were not reacting. I reached out to a friend who worked at an elder facility. He encouraged me to use the word “dementia” and to be matter-of-fact with the kids: she did not remember she was asking the same questions again or repeating stories, and there was no point to calling that out because she would not remember that either.
At the time my mom passed away, she still knew my Dad, loved talking with him about their favorite stories (which he also never tired of), and they were a good team together. He gradually managed almost all of the tasks of living, including helping her shower and dress. These days I spend time with folks who have dementia to a much more significant degree than she ever did, and I am in a different space of understanding than I was then.
The view from my front yard (L) of fractal trees covered with ice on a cloudy day. The view from my back yard (R) of icy trees illuminated by sunshine. Both have an evocative complexity and many more layers than can be reconciled.
About two weeks ago, I went to visit one of the folks I volunteer with and she was in a truly lovely, sweet mood. She was holding a baby doll, a little larger than a newborn, cuddled to her shoulder. She tucked her head to it and cooed, patted its back. She was so happy to be taking care of this baby, giving snuggles and comfort. I sat next to her and we talked in a sense. There were lucid/attached to shared reality moments within our exchanges but mostly I sat near her and enjoyed her company.
Talking with my non-binary teen about it later, they immediately cued into the energy of the moment as being the only important part. They helped me find the image of a grown-up figure holding a child-sized figure (at the top of this page) and we talked about how strange it is that much of clipart for elderly women feature someone grey-haired with a bun. There are photographs of seniors holding baby dolls online — I have since learned this is a known therapeutic activity — but my teen and I were concerned that those photographed may not have been able to truly give consent.
On Friday, I had a first meeting with someone new. She was chatty with a nervous energy in her hands, twisting her clothes. I handed her a set of fidgets and that gave us something shared to do, to look at, to turn over, to sort (with no rule, no right/wrong). She speaks in tumbled words and phrases and I respond according to tone: ‘Oh, I see’ works with both enthusiasm and empathy.
Brightly colored fidgets ‘sorted’ into a box and its lid.
At the end of my visit I said, “I am so glad I got to spend time with you.” She looked up and said, “thank you.” Telling this to my teen son later, I said there was no way for me to know if that was just a random alignment of what she said with the moment or if the social cues are so practiced as to remain intact/attached. He said, “yeah, that makes sense but it doesn’t matter. It was real.”
I wanted to share these stories from my mom to these other people’s moms in part to revisit the experience of not understanding what was happening, and how to relate to it. I am glad now to spend time talking about these relationships, finding the energy of the moment and being real together.
When I came into the facility, I saw an elderly man exposed from the behind using the raised feet of recliner chairs (that had occupants) to make his way across the room. There weren’t staff around which was unusual at this place and time of day. I went up to him and put my left arm across his shoulder and my right arm under his. I said, “Where are you headed?” He said, “bathroom.” About then a person in scrubs came up as well and snagged a community wheelchair. When my companion sat down into the seat, he got a look on his face that I suspected was the realization that his pajamas had fallen — his bare skin against the vinyl seat — but there wasn’t time to register that indignity because another one was coming if we didn’t get to the bathroom quickly enough. We did though.
As soon as he was set and the door closed, I looked up to see a woman advancing with her walker and waving in the manner attempting to get attention. I don’t know where that person in scrubs had gone. I approached and she said, “A woman has come into my room, laid on my bed and now she’s asleep. Can you help?” I said, “I can try.” She replied, “I can’t hear very well.” As I entered her room she called after me, “Please be gentle with her. I know she is tender-hearted.“
It was a nice space, sweetly decorated and inviting in style. The ‘intruder’ was sitting up just as I walked over and pulled a small blanket across a chair in the corner.
She said, “I put this here for you. Do you like it?” I said, “I do. Let’s sit together.”
She said, “here?” I responded, “Let’s find a couch. Do you like baseball?”
She said, “yes.” I sang, “Take me out to the ballgame. Take me out to the crowd…” I put my left arm around her back and my right hand under hers. She smiled and sang with me. At the nearest couch, we sat down. I sang whatever songs I could think of for a little while.
The thing is: I know all of these people some.
The man had been one of my friends in volunteering with Hospice, given a ‘live discharge’ because he was doing so well. He and his family had felt like there was a little too much hovering. That level of support may have been why he had improved though.
I had met the woman with her walker on a previous visit, new to the facility and a little shy about hanging out in the community rooms so she did not know many of her neighbors names. She truly cannot hear well so introductions may not have gone very far.
The second woman I have had interactions with previously; she had been unsettled by the strangeness of a lotus painting, but enjoyed meadow daisies. Watching her on this day, it felt like there had been a decline since I’d spoken with her last. Going into others’ rooms certainly could not be allowed (for a variety of reasons), and I felt a steeper fall in her experience of life may be forthcoming.
The first woman brought an afghan blanket and I put on my voice amplifier so that she could hear me more easily. She said I was so kind. I did not feel kind.
I felt that this is how it is sometimes. Sometimes we make it to the bathroom humanity intact and with help, other times we don’t. Sometimes we find one another in ways small and profound. Sometimes there are smiles and songs, sometimes sad.
Posted on November 3rd, 2021 by someone I do not know but whose story held significance.
Sometimes ideas are difficult to wrap our minds around — that we may have never seen someone complete a task in a particular way, so it seems unusual or difficult to try. Or, a person may have never thought about an activity they already do in an additional context.
Example: everyone I know communicates using a wide range of methods:
sounds with mouthparts (commonly speaking, but other noises as well),
facial expressions,
body movements and gestures,
visual and text media (such as sharing photos, exchanging text messages, emojis and emotional reactions, writing notes, etc.), and
references to things outside of themselves (a cardboard roll indicating there’s no more toilet paper, a family calendar or coordinating app, a glance at an empty glass to alert a waiter that more drink is wanted, and so on).
Screenshot of text exchange with one of my teens which illustrates ‘sounds,’ words, images and punctuation incorporated to convey messages.
One of my teens types out noises they might make incorporated into their messages — that’s tricky for me since they also have used acronyms to save time and keystrokes. Fortunately, I can use the emotional reaction (represented by a question mark) to convey that I am confused.
My point is: using a wide variety of approaches is not new. It’s part of how everyone communicates all of the time.
All of this also applies when it comes to someone who has dementia (changes to their thinking), or aphasia (changes to language), or does not hear perhaps as well as they once did; and even in situations that are a combination of factors.
My own experience with elder populations is that whether a listener has dementia, aphasia, or no hearing aids: yelling seems to be the most typical go-to strategy. I’m not sure why that is exactly, but it may be that’s what has been seen (with elder populations) and so that’s what gets re-tried.
It may be hard to imagine incorporating other communication methods though if you’ve never seen it before. This isn’t a perfect example, it’s just one illustration of how it might look:
I am wearing a personal amplifier with the speaker set near my friend to support hearing in a noisy environment. Holding up an item (a wreath decorated with sewing notions), allows for shared viewing and reference. A set of dry erase cards allows for quick hand-written notes or to provide options.
I have written previously on the set of dry erase “flash” cards I have in supporting exchanges. They are easy to hold in my hand and are on a ring so I can flip to a blank card readily in a conversation (without pausing to erase) or refer back to something if needed. It’s also a way for me to gauge messages that are repeated often enough to warrant making a permanent card in the set. I have used letter stickers and typed messages that I affixed with clear packing tape.
A phone’s camera can also be a ready and fast way to share information or provide a visual cue. Taking a photo of the nightstand allowed my friend to tell me what she wanted off of it:
A collection of lotion and hygiene items, personal effects, and snacks that were on a nightstand out of reach and angle of view of an individual can be photographed to present an impromptu “menu” of options.
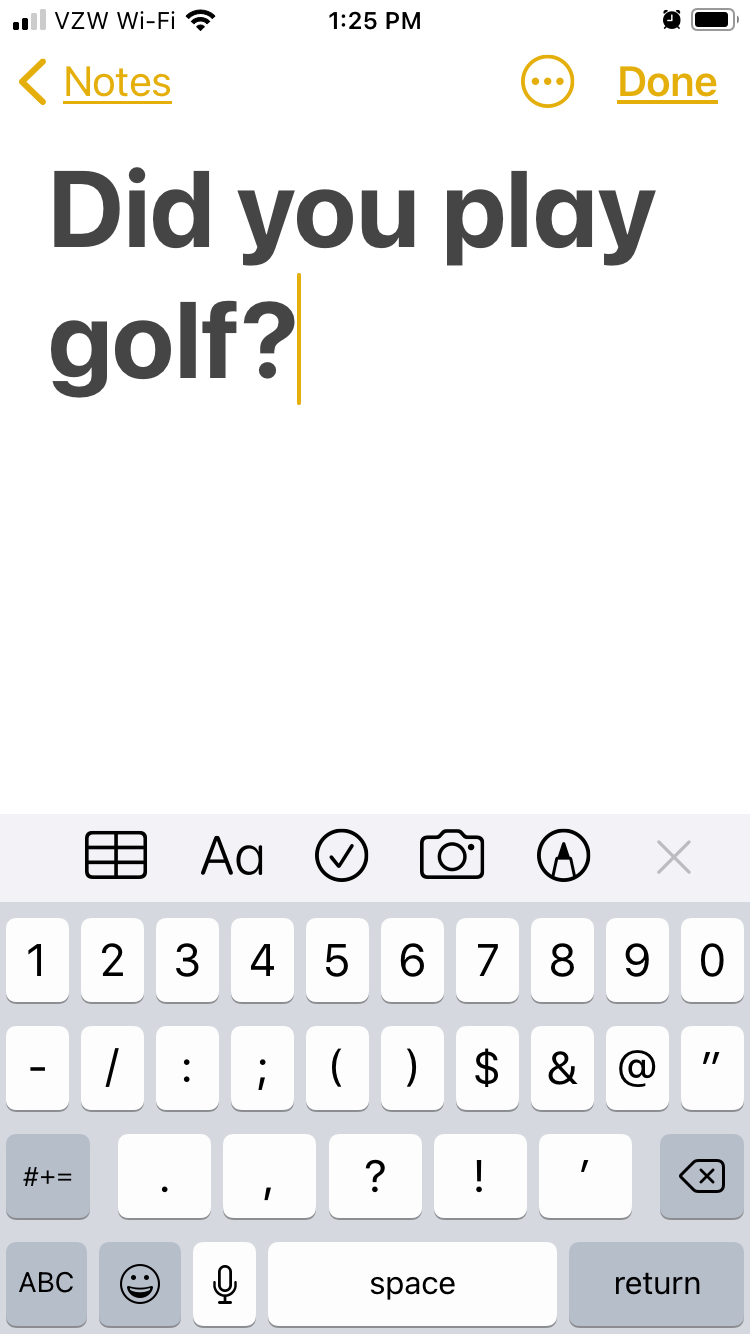
Recently I had a different opportunity to use a standard app on my phone — opening a new Notes page and typing with the largest font in bold allowed a high-contrast, backlit text support which proved more functional than my hand-written ones for an individual who has significant vision impairment.
Again, using a wide variety of approaches is not new. It’s part of how everyone communicates all of the time.My point is: to try providing examples of different ways we all already communicate in the additional context of with elder populations.
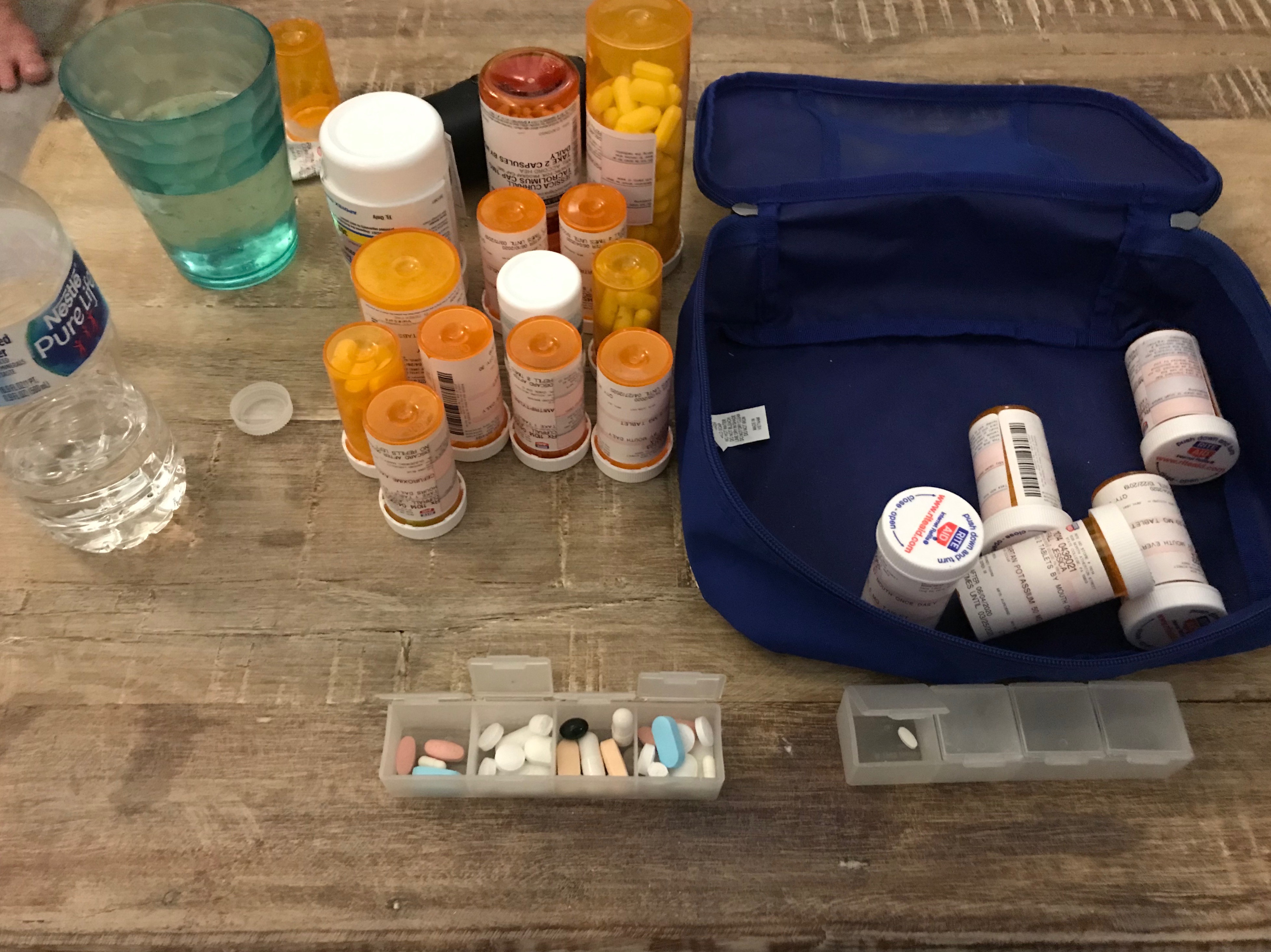
For a surprisingly long time I shared information or asked questions about my prescription management as though other people in my life also kept track of 18 different medications — not including over-the-counter (OTC) pain killers, supplements, and vitamins. It was something of a realization that I take w-a-y more pills per month (~40 x 30 = 1,200), than my spouse does collectively in a year.
When I realized that, I started trying to keep those conversations to my physicians and their teams. I bring two versions of summary tables I update with any prescription change: alphabetically by generic name which includes notes on why I am taking each, and an outline of how I take my medications across the day.
I originally tried this method because I was working with a sleep specialist and wanted to see if any of the meds I take are associated with daytime sleepiness. Then, because I already had it, I shared it with both of my nephrologists (transplant and local) and they felt like this was helpful to get a snapshot of my regimen.
Given this perspective of my day, I was described as having a “heavy pill load;” which kind of amused me insofar as I have had no fewer than 26 pills per day for over 10 years now. While this particular snapshot has more than that, at some point, what’s the difference? The gap from 26 to 40 just feels insignificant when there’s already five routine times to take meds per day. I may be able to whittle that down again, but it’s unlikely to ever return to a quantity that would be consistent with “healthy” people.
My definition of “healthy” or “normal” people are those who do not do these kinds of tasks as part of their day, or even as part of their conversations with their physician.
The thing is: there is cost and risks to not having conversations with people other than physicians and their teams.
On August 26, 2021, I went into an Outpatient Lab Facility to complete my routine bloodwork and urinalysis. As a kidney transplant recipient, that has been part of my monthly monitoring for the last decade — with the caveat that in the early days post-transplant it was every few days, and presently with the pandemic, it is sometimes more like every 6 weeks. That’s around 120 times so far and does not reflect the number of times I complete bloodwork or urine samples for other reasons; most commonly, with a suppressed immune system, I am susceptible to urinary tract and bladder infections. Are those different or two names for the same thing? It feels like I should know that, but I don’t. Also, I have a jumpy pelvic floor. With endometriosis, appendectomy, a twin pregnancy with C-section, peritoneal dialysis, and kidney transplant all in the same region surgically, I carry myself with unusual core muscle allocation. That is, I don’t always use the muscles I should and this puts stress on the muscles that are compensating that can result in spasms and cramps that feel very much like the urgency associated with a urinary tract infection (UTI).
There is no joy in learning what I really really thought was a UTI isn’t because it means:
I cannot trust my interpretation of what my body signals relay (I cannot trust myself),
I am doing it to myself: I am the reason I am in pain, and
it will be that much harder the next time I do have a UTI/bladder infection for me to recognize it.
I worked with my Occupational Therapist for pelvic floor pain relief to develop this process, which was doubly appropriate since part of the challenge was in the fine motor skills (using my hands).
The summary version of my Clean Catch Protocol is:
After I wash my hands, I tear each of three towelette packets along three of their outside edges and fold them open to try to maintain the ‘sanitary’ environment of the sealed packet.
I unfold the towelettes a little bit — only in this way are they actually usable for me.
I wipe myself down there (I’m not being coy, I actually cannot see the area I am working with), from front-to-back with each towelette separately ‘right, left, center’ and without ever letting myself ‘close’ because that would violate the whole point of cleaning. In the photo series, I used my laptop hinge to sort of illustrate this concept.
(Not pictured, even metaphorically): Pee ‘some’ into the toilet and then move a collection cup into the ‘stream’ to capture at least 30ccs.
If you’ve never peed on your own hand, it is evident that you and I live very different lives. I do not intend to be gross or crude. The thing is, part of the deal with chronic illness is accepting a level of discourse you may have never imagined for yourself. Part of coping with that, for me, is a sense of [gallows] humor. I have been greeted hundreds of times with the question, “Can you urinate for us?” If that’s not funny, it’s surreal and absurd…bordering on nightmarish.
And, as many times as I have done this, I do not understand why this is the procedure for owners of vaginas. My personal experience is that no matter how careful I am there is a HIGH probability that the sample will be considered “contaminated.” I do not know what the quantitative count of how many times that has been told to me over the years, but the emotional toll is HIGH. Is there a comparable experience quite like being told, regularly, that your every effort to be ‘clean’ with your private parts was still too dirty? The advertisers of feminine hygiene products bank on that shame.
I would also extend that this is extremely difficult to talk about. It IS gross/general or crude/rough, in part, because no one talks about it. What do persons who have more challenged motor control than I do, do with this at all? Add it all up, most importantly: How does this ever get improved upon?
I don’t just mean make it so that it isn’t awkward or embarrassing — although I would argue those are valid goals on their own — a “contaminated” result is all that it tells. There is no other additional information learned. Some of those not-a-UTIs could not be verified based on the follow-up sample; that does not mean it wasn’t a UTI. The next step in the decision-making hierarchy in that event is if I have symptoms. My aforementioned history with this pattern is a conflict of interest and credibility. Also, if this information is important, it is important to increase its success rate in providing usable results. I cannot do that on my own.
This isn’t a journal entry about my awesome specialized experience in medication management or completing Clean Catch Urine Specimens. It’s a journal entry about sharing the awkward, crude, gross, surreal, absurd, and even nightmarish with the goal that it even they can be improved upon.
What becomes normalized THEN is: Someone else will hopefully not have as complicated a time. Plus, eventually, someone else will figure out how to make things even better.
“One day you will tell your story of how you’ve overcome what you are going through now, and it will be part of someone else’s survival guide.”
While I was signing in at the front door of the personal care facility, a woman came up to me with a determined stride. She stood in the doorway and said, “What are you doing here?” I do not know if she recognized me from other times I have come (twice per week in the last two months), but it is doubtful. I am familiar with her though because she is often in the community t.v. room — not typically looking quite this uncertain.
I responded, “There are folks here that I visit.” She replied, “Can you visit me?” So I said, “Sure.”
When I stepped inside the building she asked, wide-eyed, “Can you take me home?”
In June (2021), I had the fortune of attending an Adult Children of Aging Parents (ACAP) online seminar with Dr. Edward Shaw where he presented on Managing behaviors of Alzheimer’s and other age-related dementias. Between that discussion and having read his book, I had a starting idea of how to respond to the vulnerable question of this woman.
I suggested we sit down together to talk. I showed her my name tag; she read it three times and complimented my picture. I asked her name, but she struggled with that (possibly more difficult because mine was still visible to her). She gave me consent to hold her hand and I explained that I came to sit and keep company with people. Then I took out two watercolor paintings I hoped would interest and distract-calm her.
A watercolor painting of a bright pink water lily or lotus flower.
In an abrupt shift in tone, she immediately and rapidly said, “I don’t know what that is. I don’t know what that is.” She shook her head, “I don’t know.” I responded, “It is a water lily or lotus.” Her facial expression scrunched up. “Lotus. I don’t know what a lotus is.” I said, “That’s all right. I have another.”
The second painting was sort of a field of flowers.
Watercolor painting of white, red, blue and purple flowers.
I said, “I was trying to learn how to paint daisies.” She said, calmly, “Oh, daisies.” I said she could hold onto the painting while she watched the t.v. program.
When I went to the room of my assigned visit, the t.v. was also on — appearing to be a Christmas program of some sort. She immediately smiled and turned to face me. As I sat down, I made small talk about the afghan crocheted blanket on her chair and the empty bird feeder by her window. The water lily was still at the top of my bag and I brought it out to show her.
“Ooh! I like that! I like the pink. I like that.” She touched the painted petals.
I went through my collection of things and found every image I had which included spots of bright pink — an outdated calendar image of a ladybug beneath another flower, a photograph of Christo and Jeane-Claude’s pink islands, a sunset landscape. Using a dry erase board with written options, we exchanged thoughts on how bright colors make us feel and other peaceful ideas (ocean waves, mountain snow, trees, birds). She had previously selected an Ansel Adams black and white mountain landscape beside her bed, and when I asked if she would like to swap it for the water lily she immediately agreed.
“Yes! That’s good. I like the pink. I like that.”
Next week I will bring bird seed so maybe we can watch birds at her window.
Over time my experiences have been shifting from young children in schools to elderly in hospice care. It remains as true as it ever was that I am very much learning how to listen, what to say and why. A conversation happened recently though that I thought I would write out in the hopes that it may nurture creative solutions with others.
I was visiting a woman whose diagnosis I do not know (it doesn’t really matter). When I arrived, she was asleep and since she is very hard of hearing, I anticipated that she would rest soundly. Instead of trying to talk with her, I sat down to write her a note. This was the first time she was wearing her hearing aids when I came by and maybe because of that or maybe it was just coincidence, but she woke up.
Her facial expression was confused and worried. She said, ‘I don’t have any money.” Before I could respond, she said more in a rush — much of it a jumble of sounds rather than distinct words. In the mix, I understood, “so sad,” and “but my leg is tangled.”
This is what I said in response:
My goal is to say my name every time because it is not relevant whether or not it is remembered.
I held up my i.d. badge (which also has my photo), and pointed to my name while I said it. Then I showed her a card on which I had written, “I am so glad to visit with you.” That’s something I have expressed (spoken and with this card) every time I have come.
Next I wrote, “Your leg is tangled?” I pointed at each word and read it to her twice. I showed her a card that said, “Do you have pain?” She nodded and gestured to her right leg under a blanket. The blanket was not twisted though, and nothing about her leg or foot appeared out of the ordinary (no discoloration, no swelling).
So I wrote, “Would you like your bed more up or more down?” She said yes, talked me through how to use the gizmo, and reported that it was better. I sat back down.
She said, “I’m sorry.“
I wrote and spoke, “I would like to ease your mind.“
She said, “Oh, thank you.”
Everything about her relaxed — her face, her posture, how she held her blanket. She lay back, and was asleep again before I wrote anything else. I sat with her awhile longer in case she roused again, but her breathing was regular and calm.
In turning it over in my mind, I feel like the conversation unfolded with statements and questions that were responsive to her even without understanding. That made them helpful to me also.
Still learning, how to listen, what to say, and why.